Wide Range Achievement Test: Insights & Interpretation
Apr 14, 2026

A teacher brings you a file near the end of term. The student is engaged, articulate, and clearly trying. Yet reading tasks take too long, spelling is inconsistent, or maths facts that seemed secure last month now fall apart under pressure.
In clinic, I see the same pattern from another angle. A parent says, “He understands everything when we talk, but the written work doesn’t show it.” A paediatrician asks whether this is dyslexia, attention difficulty, a learning disorder, recovery after illness, or a gap in instruction that has widened over time.
In these situations, the wide range achievement test often becomes useful. It gives us an objective look at core academic skills, quickly enough to fit into real-world school and healthcare workflows, but with enough structure to guide next decisions. It does not tell the whole story. It does tell us where to look more closely.
For teams trying to move from concern to action, that distinction matters. An achievement score can confirm that a problem is real and measurable. It can also help us avoid vague language like “not working to potential” and replace it with something clinically and educationally useful.
If you're sorting through that kind of question, this guide to an assessment for learning disabilities is a helpful companion resource. It places achievement testing in the wider process of evaluation and support planning.
Introduction When Academic Progress Raises Questions
A common referral starts with a contradiction. The student speaks well, participates in discussion, and seems bright in conversation. On paper, the work doesn’t match.
In a school meeting, one teacher may describe a reading concern. Another may focus on written output. A physician may hear about headaches, frustration, or avoidance. A psychologist may be asked a bigger question. Is this an academic weakness, a broader cognitive issue, or both?
The Wide Range Achievement Test, usually referred to as the WRAT, helps teams ground that discussion in measurable academic performance. It is one of the tools clinicians and educators use when they need a structured snapshot of reading, spelling, and maths-related skills.
That matters because struggling students are often misunderstood. Some are labelled inattentive when the main problem is decoding. Others are assumed to have a reading disorder when the deeper issue is language, memory, or processing speed. The WRAT doesn't settle every one of those questions, but it gives us a disciplined starting point.
A good assessment doesn't just describe a struggle. It narrows the possibilities and helps the team choose the next best question.
In practice, I think of the WRAT as the first clear photograph in a blurry case. Before intervention planning, before accommodation decisions, and before debates about diagnosis, we need a dependable picture of current academic skill.
That picture becomes more useful when the whole team reads it the same way. Teachers want classroom implications. Paediatricians want referral clarity. Therapists want baseline data. Parents want an explanation they can understand. The WRAT can support all of those needs when it is interpreted carefully and placed in context.
What the Wide Range Achievement Test Actually Measures
The WRAT serves as a brief check of core academic skills. It samples the basic school tasks that support later learning, then gives the team a shared reference point for deciding what needs closer study.

In practice, I describe it to school and medical teams as a screening lens for academic performance. If a child is falling behind, the WRAT helps clarify whether the strain is showing up most clearly in word reading, sentence-level reading, spelling, or written calculation. That is useful because intervention planning works best when the team can name the skill that is breaking down before debating causes, diagnoses, or placement.
For readers comparing measures across referral questions, this guide to individual achievement tests used in psychoeducational assessment helps place the WRAT alongside other academic tools.
What the WRAT-5 is built to sample
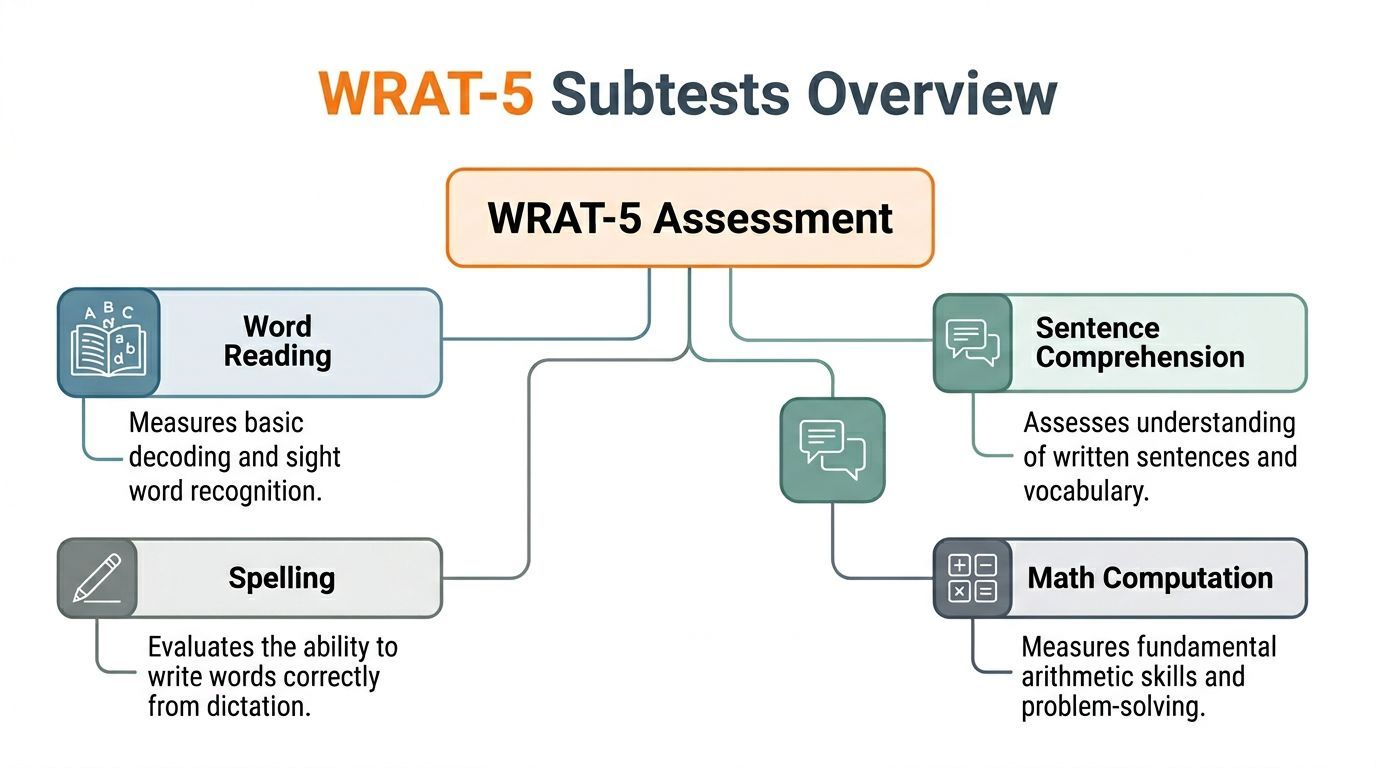
The WRAT-5 focuses on four areas:
Word Reading, which samples letter identification and single-word reading
Sentence Comprehension, which samples understanding of written meaning at the sentence level
Spelling, which samples written encoding from dictation
Math Computation, which samples written calculation skills
Those areas matter because they function like academic load-bearing walls. If one is weak, classroom performance often starts to sag around it. A student with poor spelling may avoid written work. A student with weak calculation skills may appear inattentive in maths because the effort required for each problem is too high. The WRAT helps the team locate that pressure point.
What scores can and cannot answer
WRAT scores describe current performance in specific academic domains. They do not explain the mechanism behind the difficulty.
That distinction is where teams often get stuck.
A low reading score may reflect a decoding problem. It may also sit beside weak language comprehension, reduced working memory, slowed processing, inconsistent attention, or limited instructional opportunity. The WRAT identifies the academic area that needs explanation. Other assessment methods are needed to understand why that weakness is present.
This is also why the WRAT should not be treated as a full map of learning. It does not give the broad reasoning profile of an IQ test, and it does not cover every part of academic functioning. Extended reading comprehension, written expression, problem-solving in mathematics, and higher-order learning strategies require other tools.
Why that distinction matters for care planning
A score by itself rarely changes a student's day at school. A plan does.
Consider two students with similarly low performance in reading-related tasks. One has poor word recognition and needs explicit decoding instruction. The other reads words adequately but loses meaning because attention fades and verbal working memory is overloaded. On paper, both students may look like weak readers. In treatment planning, they need different supports.
Pairing methods improves decision-making in these situations. The WRAT shows the team where the academic breakdown appears. A digital cognitive platform such as Orange Neurosciences can help examine attention, memory, processing efficiency, and other functions that may be driving that pattern. Together, those data move the conversation from "the student is behind" to "here is the likely barrier, and here is the support plan that fits it."
Practical rule: Use the WRAT to define the academic problem. Use cognitive and clinical assessment to identify the processes contributing to it.
A Deeper Look at the WRAT-5 Subtests and Scoring
A WRAT-5 report can look deceptively simple. Four subtests, several score types, and a short administration time can make the results seem straightforward. In practice, interpretation is more like reading a set of vital signs. The numbers show where academic performance is strained, but they do not explain the cause. That distinction matters if the goal is a useful intervention plan rather than a descriptive label.
The four subtests in plain language
The WRAT-5 samples four academic skill areas that schools and clinics often need to check quickly.
Subtest | Task | Primary Skill Measured |
|---|---|---|
Word Reading | Identify letters and read words aloud | Basic decoding and word recognition |
Sentence Comprehension | Complete sentences using a modified cloze format | Understanding written meaning in context |
Spelling | Write letters or words from dictation | Encoding sounds and written spelling accuracy |
Math Computation | Solve written maths problems | Calculation and written computation skills |
A broader comparison of brief and extended achievement batteries appears in this guide to the WIAT achievement test. That comparison helps teams choose the right tool for the referral question instead of assuming every academic concern needs the same depth of testing.
Word Reading
Word Reading examines how accurately a student can identify letters and read increasingly difficult words aloud. It is a direct look at print recognition. For younger children, that starts with letters. For older students, it becomes a graduated sample of single-word reading.
Clinically, I treat this score as an entry point into the reading system. A low result raises questions about decoding development, phonics instruction, reading fluency, and how much effort the student spends just identifying words. If word recognition is slow or inaccurate, comprehension problems often follow for reasons that have little to do with higher reasoning.
Sentence Comprehension
Sentence Comprehension often changes the discussion in team meetings.
The student fills in missing words in written sentences. That means the task draws on reading accuracy, vocabulary, syntax, and enough attention to hold the sentence together while selecting a word that fits. A student can look adequate on isolated word reading and still struggle here because sentence-level meaning places a heavier load on language and working memory.
That pattern is clinically useful. It tells the team to ask whether the difficulty sits in language comprehension, sustained attention, reading efficiency, or a mix of all three.
Spelling
Spelling gives a different window into literacy. Reading asks the student to recognize a printed word. Spelling asks the student to build it.
That difference matters. Dictated spelling depends on phonological awareness, sound-symbol mapping, stored orthographic patterns, and written output. Students with weak spelling sometimes sound far more capable than their written work suggests. In those cases, the score can help explain classroom frustration, slow written production, and avoidance of tasks that require independent written language.
For some families, this is the first score that makes the problem feel concrete. It connects the complaint of "he knows it when he says it" to an observable weakness in encoding.
Math Computation
Math Computation measures written calculation skill across a range of problem types. The focus is accuracy in computation, not broad mathematical reasoning or verbal explanation.
That distinction prevents a common misunderstanding. A student may understand quantity, patterns, or problem-solving concepts during discussion and still produce weak computation because of fact retrieval problems, sequencing errors, inattention, or visual organization difficulties on the page. In care planning, those are very different intervention paths.
How long the WRAT-5 takes
The WRAT-5 is often chosen because it can be administered efficiently in school, pediatric, rehabilitation, and psychology settings. That efficiency makes it useful as a screening or follow-up tool, especially when the team needs a quick academic snapshot before deciding whether broader testing is necessary.
Short tests have tradeoffs. They are good at identifying where concern is concentrated. They are less helpful for explaining why the weakness appears.
What the scores mean
Score interpretation is where many smart teams drift into overconfidence. A number looks precise. Clinical meaning still depends on context.
Standard scores
Standard scores compare performance with age-based expectations. The average score is set at 100, with predictable distance above and below that point.
A score near the average range suggests performance is broadly in line with same-age peers. A meaningfully lower score signals that the skill needs attention, especially if the weakness matches referral concerns, classroom observations, or a decline from what the student shows in conversation. A higher score can be equally informative. It may reveal a genuine strength or a split profile that deserves explanation.
The practical question is simple. Which academic skill is weaker or stronger than expected, and what should the team do because of that pattern?
Percentile ranks
Percentiles are easier for many families to grasp because they answer a familiar question: how many peers performed below this student? They are useful, but they can also sound more dramatic than they are.
A low percentile does not tell us what process broke down. It only tells us where the student's performance falls relative to peers. That is why I rarely discuss percentiles without linking them to classroom function and to other assessment results.
Age and grade equivalents
Age and grade equivalents are descriptive shortcuts, not placement decisions. They can help families picture the level of items the student managed, but they are easy to misread.
If a child earns a grade-equivalent score below current placement, the team should not conclude that the child is functioning like a student in that grade across all learning tasks. The safer interpretation is narrower: performance on this type of item resembles that of students at that level in the norm sample. For intervention planning, that is a starting point, not a conclusion.
Retesting and alternate forms
The WRAT-5 includes alternate forms, which can help with repeat testing when the team needs to monitor change over time. That is useful in rehabilitation, short-term intervention follow-up, and some school-based reviews.
Still, repeated achievement scores should be interpreted carefully. If a student improves, the next question is whether instruction changed the academic skill itself, whether attention and stamina improved, or whether both happened together. Pairing WRAT findings with digital cognitive testing can answer that second question more clearly. Orange Neurosciences' platform is especially helpful when a low WRAT score needs explanation in terms of attention, memory, processing efficiency, or executive control.
That combined approach also helps in more complex presentations, including students who appear advanced in some areas and unexpectedly weak in others. Teams discussing enrichment, twice-exceptionality, or outside supports sometimes look at resources such as gifted and talented test practice, but achievement data still needs careful interpretation. A high-ability student with one low WRAT subtest does not need a generic plan. The team needs to identify the specific academic weakness, then test the cognitive processes that may be interfering with performance.
How Professionals Use WRAT Results in Practice
Scores only matter if they change what the team does next. In day-to-day work, the WRAT is most valuable when it sharpens the intervention plan.

A dyslexia referral in paediatrics
A developmental paediatrician refers a child because reading has lagged behind spoken language for years. The family says the child is verbal, curious, and strong in discussion, but reading is slow and tiring.
WRAT results show weak Word Reading and reduced Sentence Comprehension relative to what the team expected from classroom participation. That doesn't diagnose dyslexia on its own. It does support the clinical concern that the reading problem is specific enough to warrant a fuller literacy and cognitive work-up.
At that point, the paediatrician may coordinate with psychology, speech-language services, or school staff to examine phonological skills, language, and broader learning history. The WRAT has done its job. It has moved the conversation from “he struggles with reading” to “these are the specific reading-related skills that require explanation.”
For families of high-ability students, confusion often runs in the opposite direction. A child may seem advanced in some areas while still having a very real academic weakness. In those cases, broader context matters, and resources such as gifted and talented test practice can help families understand why strong reasoning or enrichment readiness doesn't rule out a reading or maths-related difficulty.
An IEP meeting focused on maths
An educational psychologist is asked to support an Individual Education Plan for a student whose classroom maths performance is slipping. Teachers report effort and participation. Written work is inconsistent, and timed tasks are especially fragile.
The WRAT Math Computation score provides a standardised indicator that the difficulty isn't just anecdotal. That helps the school team justify targeted numeracy support, explicit review of foundational calculation procedures, and accommodations for task load or written output if needed.
The value here isn't only the score. It is the shift from general concern to specific planning.
A useful meeting discussion sounds like this:
What is weak: written computation accuracy
What still needs clarification: number sense, visual organisation, working memory, or attention under task demands
What to change now: direct skill instruction, scaffolded worksheets, shorter sets with immediate feedback, and progress checks
That is a much stronger care plan than “try harder in maths.”
A rehabilitation baseline after brain injury
In rehabilitation settings, I often see the WRAT used differently. Here the question isn't always a developmental learning disorder. Sometimes the team needs a clean academic baseline after injury, illness, or neurological change.
A therapist may use WRAT-5 to document current reading, spelling, and maths-related functioning as part of return-to-school or return-to-work planning. Because the test has alternate forms and supports retesting over a short interval, it can help the team track whether academic skills are stable, recovering, or declining across treatment blocks.
The broader meaning of those results usually depends on the rest of the evaluation. This overview of what is neuropsychological assessment is useful for teams that need to place academic scores within attention, memory, executive functioning, and recovery planning.
Turning results into concrete recommendations
In school and healthcare settings, I encourage teams to translate WRAT findings into three categories.
What to teach directly
If Word Reading is weak, direct work may focus on decoding, word recognition, and structured reading practice.
If Spelling is weak, intervention may target phoneme-grapheme mapping, spelling patterns, and written encoding.
If Math Computation is weak, support may involve explicit calculation routines, visual layout support, and cumulative review.
What to accommodate
Instruction takes time. Students often need support while skill-building is underway.
Examples include:
Reduced written load when spelling or sentence-level reading is a barrier
Oral presentation of instructions when print access is slowing task completion
Extra time when basic academic processing is effortful
Alternative demonstration of knowledge when the bottleneck is written output rather than understanding
What to investigate next
This is the step teams skip most often.
A low WRAT score should prompt a question about mechanism. Is the student missing instruction? Is reading effortful because of decoding weakness? Is sentence comprehension low because of language or attention? Is maths fragile because of memory, sequencing, or visual-spatial organisation?
The most useful WRAT interpretation isn't “this score is low.” It's “this score tells us which intervention to start and which mechanism still needs clarification.”
Understanding the Strengths and Limitations of the WRAT
The WRAT has lasted because it solves a real problem. Teams need a brief, structured, well-established way to measure core academic skills. The test does that well.
It also has clear limits. Good interpretation depends on respecting both sides.
Where the WRAT is strong
The first strength is efficiency. In schools, clinics, and rehabilitation settings, there is value in a test that can be administered without overwhelming the student or the schedule.
The second strength is reliability. Reliability asks a simple question. If we measure the same kind of skill carefully, can we trust the score to be stable enough to guide decisions?
For the WRAT, the answer is strong. Split-half reliability coefficients reported for the test reached .98 for Reading, .94 for Arithmetic, and up to .97 for Spelling (Wide Range Achievement Test overview). Those values support its use as a dependable academic measure.
The third strength is clarity of focus. The WRAT measures basic academic performance, not everything at once. That narrowness is often an advantage when the team needs a quick read on whether concerns in reading, spelling, or computation are objectively present.
Where the WRAT can mislead if overused
The test becomes less helpful when people ask it to answer questions it was never built to answer.
A low reading-related score does not automatically identify the cause. A low maths-related score does not separate conceptual weakness from attentional breakdown or visual organisation problems. A spelling weakness does not tell you whether the underlying issue is phonological, orthographic, motor, or instructional.
The WRAT also isn't a full measure of:
Extended reading comprehension
Written expression
Mathematical reasoning
Broad cognitive functioning
Emotional or behavioural contributors to performance
That means a very neat WRAT report can still leave the most important clinical question unanswered.
The car analogy holds up
If the WRAT tells you the engine is misfiring, that is valuable. You still need a mechanic to tell you whether the problem comes from fuel delivery, ignition, compression, or something else entirely.
In the same way, the WRAT identifies where academic performance is breaking down. It doesn't fully explain the system behind that breakdown.
A useful way to evaluate score confidence is through the broader concept of test-retest reliability, especially when teams are using repeated measurement to judge whether intervention is helping.
Use the WRAT when you need a reliable academic snapshot. Don't use it as a shortcut around a fuller differential assessment when the referral question is complex.
A balanced clinical takeaway
If the referral question is, “Are there measurable weaknesses in foundational academic skills?”, the WRAT is often a very good choice.
If the referral question is, “Why is this student struggling, and what specific mechanism should treatment target?”, the WRAT is only part of the answer.
That isn’t a weakness in the test. It’s a reminder to use the right tool for the right job.
Pairing WRAT Results with Modern Cognitive Assessments
A familiar case illustrates the gap. A student is attentive in conversation, participates well in class, and seems to understand lessons aloud. Then the WRAT shows weak Sentence Comprehension and Spelling. The team now has proof of an academic problem, but the treatment plan is still incomplete.
The WRAT answers the first question. It shows which learned skills are below expectation. The next question is the one that shapes care: what is getting in the student's way during reading, writing, or maths tasks?

From score pattern to treatment target
For a multidisciplinary team, the WRAT works like a symptom screen in medicine. It identifies the area of concern. A cognitive assessment helps identify the process behind that concern.
A low Word Reading score can reflect different underlying problems. One student may struggle with phonological processing. Another may decode accurately but work so slowly that comprehension falls apart. A third may have inconsistent attention, which makes performance uneven across tasks and settings. Those students can earn similar achievement scores and still need different interventions.
The same logic applies to maths. A weak Math Computation score does not automatically mean the student needs more drill work. The barrier may involve working memory, sequencing, visual organisation, or mental fatigue under sustained effort. If we treat all of those profiles as the same problem, we usually get partial progress and a lot of frustration.
Why pairing matters in current practice
More teams now assess students across school, clinic, and remote settings, and Pearson notes growth in telepractice as part of its WRAT-5 product information (Pearson Assessments WRAT-5 product page). That shift matters because follow-up decisions often need to happen quickly, with data that can be reviewed over time rather than filed away after a single visit.
This is one reason many clinicians pair a traditional achievement test with a digital cognitive platform such as Orange Neurosciences. The WRAT shows the academic output. A modern cognitive assessment can clarify whether the student is being limited by attention control, processing speed, working memory, executive regulation, or visual-motor load. That pairing gets the team closer to the why.
What the combined profile looks like
Consider a student with low Sentence Comprehension and Spelling scores, but strong verbal discussion in class. Without more assessment, the plan may default to extra reading practice and weekly spelling review.
A cognitive profile can sharpen that plan by showing patterns such as:
Working memory weakness, which makes it hard to hold sentence parts in mind long enough to interpret meaning
Slow processing speed, which turns reading into a laborious task and reduces fluency
Attention variability, which produces inconsistent written performance across the day
Visual-motor or output strain, which interferes with spelling and written production even when ideas are intact
Now the intervention plan changes in a practical way. The teacher may shorten written directions, the psychologist may recommend supports for task initiation and sustained attention, and the physician or therapist may look more closely at fatigue, medication timing, or motor demands. Families can also match home practice to the actual bottleneck instead of increasing homework volume. Resources on most effective study techniques can be useful here, but only after the team knows which cognitive demands are limiting performance.
How each discipline uses the pairing
Educators can connect accommodations to the student's actual barrier. A child with intact reasoning but weak working memory may need reduced written load and stepwise instructions. A child with a primary decoding weakness needs direct reading instruction.
Healthcare providers gain a clearer referral path. If the WRAT shows academic weakness and cognitive testing points to attention or executive difficulties, the next recommendation becomes easier to explain and easier for families to act on.
Rehabilitation teams also benefit. After concussion, neurological illness, or injury, achievement scores may improve before cognitive endurance returns. A student can read better on a brief test and still struggle with full school days because speed, fatigue control, or planning remain below baseline.
A workflow that keeps the plan grounded
A practical sequence usually looks like this:
Use the WRAT to identify the academic skill area that is weak
Add cognitive assessment to test likely mechanisms behind the weak performance
Write interventions that address both the academic deficit and the process barrier
Repeat selected measures to check whether the barrier is changing
That final step matters. If spelling improves only when tasks are shortened, the team has learned something different from a case in which spelling improves because working memory and attention control also improve.
The main advantage of pairing these tools is clarity. Achievement testing keeps the discussion tied to school performance. Cognitive testing helps the team choose supports that fit the student's actual pattern of difficulty. That is how a WRAT score becomes the start of an intervention plan rather than the end of an evaluation.
Your Actionable Plan for Using Achievement Data
If you're using the wide range achievement test in school, clinic, or rehabilitation work, the goal isn't to gather another score. The goal is to make the next step clearer.
When to request or refer for WRAT assessment
Consider a WRAT when:
Progress and effort don't match and the student appears to work hard without corresponding academic gains
Reading, spelling, or maths concerns are recurring across settings and reports
A baseline is needed before intervention, accommodation planning, or return-to-school decisions
The team needs objective academic data instead of general impressions
Questions to ask when you receive the results
A strong case discussion usually includes these questions:
Which academic skill is weakest right now
Does the score pattern fit the concerns reported by teachers and family
What can we start teaching differently this week
What still needs deeper assessment
Which accommodations are justified while intervention is underway
Those questions keep the WRAT connected to action.
How to advocate for a fuller profile
If the WRAT confirms weakness, don't stop there when the referral question is complex.
Ask whether the team has enough information about:
Attention
Working memory
Processing speed
Executive functioning
Visual-motor or output demands
That fuller profile often determines whether support is well targeted or well intentioned.
For families and older students, practical study guidance can also help support the intervention plan between appointments. A resource on most effective study techniques can be a useful add-on when the team is trying to translate assessment findings into everyday routines at home or school.
The shortest useful checklist
Get the academic baseline
Identify the weakest functional skill
Ask what mechanism may be driving it
Start targeted intervention
Add accommodations immediately if the barrier affects access
Reassess to see whether the plan is working
When teams follow that sequence, WRAT data become much more than a score report. They become a decision tool.
If you want to build a more complete picture than academic scores alone can provide, explore Orange Neurosciences. Their platform helps clinicians, educators, and families add rapid cognitive profiling to the assessment process so intervention plans can address not just what is hard, but why it is hard. You can visit the site to learn more, request a demo, or contact the team directly about creating more actionable student and patient profiles.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation