Mastering Patient Health Questionnaire 9 Interpretation
Mar 24, 2026

When you're with a patient, what does that PHQ-9 score actually mean? Beyond the number, what does it tell you about their experience, and more importantly, what should you do next?
The PHQ-9 is one of our best frontline tools for getting a quick, evidence-based snapshot of depressive symptoms. But a score is just data. Our job is to translate that data into a meaningful clinical story and a clear plan of action.
From Score to Severity to Action
Think of the total PHQ-9 score as a clinical traffic light. A low score might be a green light, suggesting things are okay for now. A moderate or high score, however, is a yellow or red light, signalling that we need to slow down, pay close attention, and decide on the right intervention.
This system gives us a consistent, reliable starting point. It helps make sure that a patient's distress doesn't get missed in a busy clinic day, turning their subjective feelings into a number that guides our immediate response.
To make this crystal clear, here’s how a raw score maps onto a severity level and a suggested clinical action.
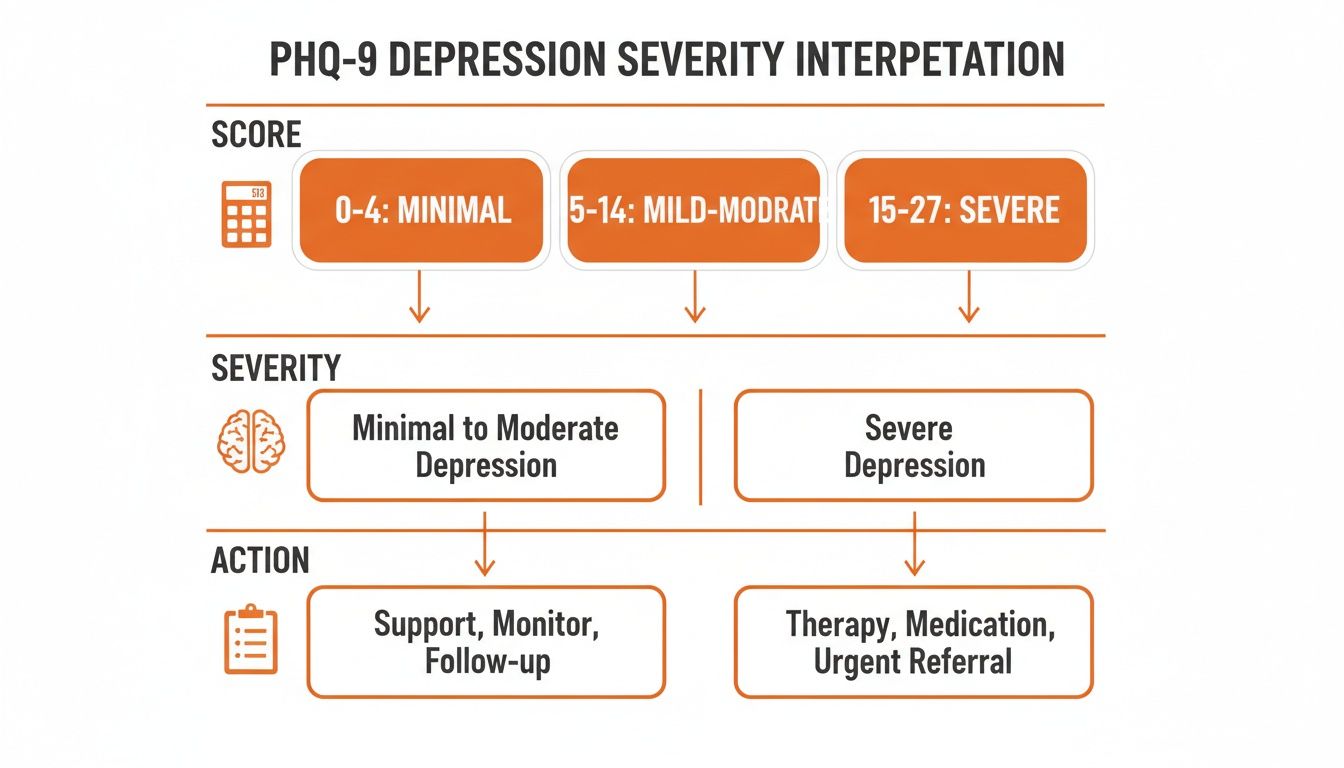
This visual guide is perfect for a quick-glance reference when you're in the middle of a patient visit and need to make a fast, informed decision.
PHQ-9 Score and Clinical Actions At a Glance
While the infographic is a great summary, sometimes you need the details laid out. The table below offers a straightforward reference, mapping the total score ranges to their severity level and our proposed next steps. It gives you the essentials in a clear, organized format.
Total Score | Depression Severity | Proposed Clinical Action |
|---|---|---|
0-4 | Minimal Depression | No action is typically needed. The score falls within a normal, healthy range. |
5-9 | Mild Depression | Use your clinical judgment. This often calls for "watchful waiting," with a repeat PHQ-9 at the next follow-up. |
10-14 | Moderate Depression | It's time to consider a treatment plan. This could involve counselling, more frequent follow-ups, or pharmacotherapy. |
15-19 | Moderately Severe Depression | Active treatment is strongly recommended, usually involving pharmacotherapy and/or psychotherapy. |
20-27 | Severe Depression | Warrants immediate initiation of treatment, combining pharmacotherapy and psychotherapy. A thorough safety assessment is critical. |
Remember, this table is a guide, not a rigid set of rules. Your clinical judgment—backed by the patient’s history, context, and your therapeutic relationship—is always the most important factor in any treatment decision.
Understanding these score ranges is the foundational first step. To see how the PHQ-9 fits into a wider diagnostic toolkit, feel free to explore our guide on other valuable mental health screening tools.
Translating Scores Into Patient Stories
A PHQ-9 score gives you a critical piece of data, but that number on its own doesn't tell you the whole story. The real art of interpretation is connecting that raw score to a person's lived experience. It’s the difference between seeing a "16" on a chart and understanding that your patient "can barely get out of bed and nothing brings them joy anymore."
This is where your clinical skill takes a simple screening tool and turns it into a powerful conversation starter. The score isn't a final diagnosis; think of it as an invitation to uncover the narrative behind the numbers. When you understand what each severity level actually feels like for a patient, you can make far more empathetic and effective decisions.
Minimal to Mild Symptoms (Scores 0-9)
A score in the 0-4 range (minimal) usually reflects the normal, fleeting dips in mood everyone has now and then. The person is likely functioning well, and the symptoms aren't causing any real distress in their daily life.
But when a score lands in the 5-9 range (mild), you start hearing the first quiet whispers of a struggle. This isn’t debilitating depression, but it's a clear signal that something is off.
Practical Example (Score 8): A patient, let's call him Mark, scores an 8. When you dig a little deeper, he says, "I just feel completely drained. It’s harder to focus at work, and I’m definitely more irritable with my family than usual." He’s still hitting his deadlines and getting through the day, but the effort it takes is noticeably greater. This score prompts "watchful waiting" and opens the door for a conversation about stress management or lifestyle adjustments. This is an actionable insight: the score isn't high enough for immediate medication, but it's a clear signal to intervene with preventative strategies.
Moderate Symptoms (Scores 10-14)
A score in this range points to a clear and persistent problem. The patient's symptoms are no longer just a background hum; they are actively interfering with work, their social life, and even basic self-care. This is a crucial threshold where intervention often becomes necessary.
This is also where we see the individual story connect with broader population data. In California, where the PHQ-9 has become a cornerstone of primary care, one study analyzed over 25,000 patient records from the state's Medi-Cal program. It found that 28.5% of screened adults scored 10 or higher, indicating moderate to severe depression. You can explore the full analysis of PHQ-9 usage in California's healthcare system. This shows just how often clinicians are faced with patients at this critical juncture.
Practical Example (Score 13): Sarah, a university student, scores a 13. She tells you, "I've stopped going to my morning classes because I can’t sleep and feel exhausted all the time. I used to love painting, but I haven't picked up a brush in weeks." Her grades are slipping, and she’s started avoiding calls from friends. Actionable Insight: Her story paints a clear picture of moderate functional impairment. The score of 13 is your cue to move from watchful waiting to active treatment, like initiating a referral for therapy and discussing potential medication options.
Severe Symptoms (Scores 15-27)
When scores climb into the 15-19 range (moderately severe) and the 20-27 range (severe), the patient's story is almost always one of significant suffering and daily crisis. Functioning is profoundly impaired, and the risk of self-harm is a serious concern that you must address immediately.
These scores demand urgent, comprehensive action. The narrative is no longer about feeling "off" but about being completely overwhelmed.
Moderately Severe (15-19): Patients here might describe missing multiple days of work, struggling with basic hygiene, and feeling a deep, pervasive sense of hopelessness. Their world has shrunk, and joy feels like a distant memory.
Severe (20-27): At this level, a patient might say, "I feel like a burden to everyone. Getting out of bed feels like climbing a mountain, and most days I just can't do it." Their answers often reveal profound anhedonia, psychomotor changes (either agitation or slowness), and overwhelming feelings of worthlessness.
This is the point where a comprehensive plan isn't just a recommendation—it's essential. Listening to these narratives is the foundation of all effective treatment and is a core principle of delivering excellent client-centred care. By truly hearing the story behind the score, you can build trust, foster collaboration, and tailor an approach that meets the person where they truly are.
Looking Beyond the Total Score to Individual Items
A total score on the Patient Health Questionnaire-9 gives you the big picture—it tells you that a problem likely exists and helps gauge its overall severity. But to truly understand what's happening, you have to look closer. Think of it as moving from a diagnosis to a story. The real art of PHQ-9 interpretation lies in digging into the individual items. This is where you uncover the unique texture of a patient's depression.

The total score tells you a storm is brewing. The item-level analysis is like checking the weather radar. Is the main threat high winds, heavy rain, or lightning? Each one demands a different response, and the same is true for a patient’s symptoms.
The Critical First Stop: Question 9
Before you look at anything else, your eyes must go directly to Question 9: "Thoughts that you would be better off dead or of hurting yourself in some way." Any positive response here, even a "1" for "Several days," is a critical alert. It requires your immediate and full attention.
A positive answer on this item isn't a moment for assumption; it's a clear signal to pause and begin a compassionate, direct safety assessment. Your primary goal is to determine the level of risk without judgment.
A positive response on Question 9 is the single most important finding on the PHQ-9. It shifts the clinical priority from screening for depression severity to assessing for immediate patient safety.
Actionable Insight: Don't just note a positive response; act on it immediately. Your workflow should treat a positive Q9 as a "stop everything" moment to assess safety. Ask a series of straightforward, non-judgmental questions to clarify risk:
Clarify the Thought: "Thank you for sharing that with me. Can you tell me more about those thoughts?"
Assess Intent: "Have you been thinking about ending your life?"
Evaluate a Plan: "Have you thought about how you might do this?"
Check for Means: "Do you have access to the things you would need to carry out that plan?"
Determine Timeline: "Have you thought about when you might do this?"
This direct line of questioning is vital. The evidence is clear: asking someone about suicide does not plant the idea or increase risk. It's one of the most important steps we can take to prevent it.
Identifying Symptom Clusters
Beyond the crucial safety check of Question 9, the other items on the PHQ-9 help you map the patient’s personal experience of depression. You'll start to see patterns that point toward either cognitive-affective symptoms (the "thinking and feeling" parts) or somatic symptoms (the physical side).
Cognitive-Affective Symptoms:
Question 1: Anhedonia (little interest or pleasure)
Question 2: Depressed mood (feeling down, depressed, or hopeless)
Question 6: Feelings of worthlessness or guilt
Question 7: Trouble concentrating
Question 8: Psychomotor changes (moving slowly or being fidgety)
Somatic Symptoms:
Question 3: Trouble with sleep
Question 4: Feeling tired or having little energy
Question 5: Poor appetite or overeating
Practical Example: One patient might score highly on questions 1, 2, and 6, showing a deep struggle with hopelessness and low self-worth, but have no issues with sleep or appetite. Another patient with the exact same total score might primarily endorse fatigue, sleep disruption, and appetite changes. Actionable Insight: These different profiles demand different approaches. The first patient may benefit most from cognitive therapy targeting negative thought patterns, while the second might see more improvement from behavioural activation focused on re-engaging with daily routines and activities.
This is also useful for differentiating from other conditions. For more on this, you can check out our guide on the Perceived Stress Scale, which measures general stress rather than specific depressive symptoms.
This patient health questionnaire-9 interpretation allows you to go beyond a generic label and start personalizing your approach. This item-level analysis is what moves you from a general diagnosis to a truly personalized strategy.
Integrating PHQ-9 Results Into Your Daily Workflow
Interpreting the PHQ-9 is one thing; actually weaving those insights into your daily clinical practice is another. How do you stop it from being just another piece of paperwork and turn it into a tool that genuinely informs your care, moment by moment? It all comes down to building a smart, seamless workflow that gets you the right information at the right time.
Practical Example: Imagine your patient checks in and completes the PHQ-9 on a clinic tablet. By the time you walk into the exam room, their score is already populated in the electronic health record (EHR). You immediately have a baseline, a flag on any critical items like Question 9, and a real-time snapshot of their mental state before the conversation even begins.
This simple step shifts the PHQ-9 from a retrospective chore to a proactive clinical instrument. It means you start the appointment with more insight, ready to focus on what truly matters to the patient. Of course, as we integrate these digital tools, it’s vital to champion digital accessibility in healthcare to ensure every patient can participate fully.

From Initial Score to Tracking Progress
The PHQ-9 isn't a one-and-done screening. Its real power comes alive when you use it to map a patient’s journey over time. Tracking scores at regular intervals, say every 4-6 weeks during active treatment, gives you objective data on how well your plan is working.
A solid benchmark for a clinically meaningful improvement is a 5-point decrease in the total score. This isn't an arbitrary number; it represents a tangible shift in their symptom burden.
Actionable Insight: This tracking method transforms your follow-ups. Instead of asking vaguely, "So, are you feeling any better?" you can say, "Your score has dropped by six points since our last visit, which is a fantastic sign. Let's talk about what's been working and what's still a struggle." It grounds your conversation in concrete data, making your clinical decisions that much sharper and helping the patient see their own progress.
Connecting Subjective Reports to Objective Data
One of the most powerful ways to use the PHQ-9 is as a launchpad for deeper, objective assessment. When a patient scores high on a specific item, it's a clear signpost telling you exactly where to dig deeper.
Let's take Question 7, "Trouble concentrating on things, such as reading the newspaper or watching television." This is a subjective report of a cognitive issue. It’s incredibly valuable, but it doesn't tell you the why or the how. Is this a problem with sustained attention? Processing speed? Working memory?
Actionable Insight: This is the perfect moment to move from a subjective feeling to an objective measurement. A high score here should be a trigger to use a tool like Orange Neurosciences' OrangeCheck, which can deliver a rapid and precise cognitive profile. This data allows you to craft a truly personalized care plan that addresses both emotional and cognitive symptoms, dramatically improving the continuity of care you provide. Suddenly, a simple questionnaire becomes the gateway to data-driven, holistic treatment.
This integrated approach isn't just theoretical; it's backed by powerful data. For example, historical data from California's rehabilitation centres revealed that while severe PHQ-9 scores (15+) were linked to 42% longer rehab stays, the facilities that used PHQ-9 scores to guide cognitive assessments actually reduced stay lengths by 18%. This is a testament to how tools that correlate processing speed with PHQ-9 items—like concentration difficulties—can drive fundamentally better outcomes.
Navigating Nuances in Patient Populations
When we look at a completed PHQ-9, it's tempting to focus just on the final score. But to truly understand what's happening with a patient, we have to look beyond the number and see the whole person. The score is a starting point, a powerful one, but the context is everything.
Think of the PHQ-9 as a powerful lens. To get a clear picture, you have to adjust the focus for each individual. Things like age, cultural background, and other health issues can completely change how symptoms show up and what they really mean. It’s a fantastic assistant, but it never, ever replaces your clinical judgment.
Age-Related Symptom Presentation
Depression doesn't present the same way in a teenager as it does in an older adult. If we don't recognize these differences, we can miss a diagnosis that’s hiding in plain sight.
Practical Example (Adolescents): A teenager's PHQ-9 might be high on irritability and low mood, but what parents report are behavioral issues and social withdrawal. Actionable Insight: Use the score to open a conversation about their feelings, framing it less as "depression" and more as "feeling angry or overwhelmed."
In older adults, the picture shifts entirely. Here, depression often shows up as physical complaints or a kind of cognitive fog.
Somatic Complaints: An older patient might come in talking about unexplained fatigue, constant aches, or sleep that just isn't restful.
Cognitive Fog: They might report serious trouble with concentration or memory. This is a big one, as it can be quickly misinterpreted as early signs of dementia instead of what it might be: depression.
Cultural and Linguistic Nuances
Culture is the lens through which we all experience and express emotional distress. In some cultures, openly talking about sadness or guilt is discouraged, so patients may focus almost entirely on physical symptoms. Their PHQ-9 might be heavy on items about sleep, energy, and appetite, but very light on the questions about mood.
Actionable Insight: When you see a high score on somatic items but low scores on emotional items, consider cultural context. Frame the discussion around the physical symptoms they endorsed. Using a validated, culturally-adapted translation of the PHQ-9 isn't just a good idea—it's non-negotiable. When working with diverse populations, getting the full picture, including an accurate medical history in Spanish, is absolutely critical.
Differentiating From Chronic Medical Conditions
This is one of the trickiest parts of interpreting a PHQ-9. A patient with congestive heart failure will almost certainly endorse "feeling tired or having little energy" on Question 4. But is that fatigue from their heart, or from a co-occurring depression?
Teasing these apart requires skillful questioning. Your goal is to understand the nature of the symptom, not just its presence.
Actionable Insight: When a patient with a chronic illness reports fatigue, ask targeted follow-up questions:
"Tell me about this fatigue. Is it different from the usual tiredness you feel from your [medical condition]?"
"When you feel this tired, have you also lost interest in things you normally enjoy?"
"Does the fatigue seem to lift, even for a little while, when you're doing something that really engages you?"
Fatigue from depression often travels with anhedonia and hopelessness. Fatigue from a medical condition might not. Mastering these nuances is what allows you to use the PHQ-9 with the precision it was designed for, making sure you’re treating the right problem.
From Screening to Measurement: The Next Step in Data-Driven Care
So, you’ve got the hang of the PHQ-9. You can read the score, you see the story it tells, and you’re starting to spot the patterns in your patients' responses. That's a huge step. But where do you go from here to provide truly data-driven care? This is how you build the bridge from subjective screening to objective assessment.
The PHQ-9 is an indispensable tool. It’s often our first, most reliable signal that something is wrong, and it’s brilliant for tracking a patient’s emotional state over time. But it has a critical limitation: it’s based entirely on what the patient tells us.
The Limits of a Subjective Story
When a patient scores high on an item like "trouble concentrating," you know there's a fire, but you don't know the source of the smoke. Is it an issue with sustained attention? A deficit in working memory? Or maybe a lag in processing speed? The PHQ-9 can't tell you that.
Relying solely on a subjective questionnaire for cognitive symptoms is like trying to diagnose a vision problem by only asking, "Is the world blurry?" To write the right prescription, you need to use an eye chart to get objective data.
Closing the Gap With Objective Measurement
When a PHQ-9 score flags a cognitive concern, your actionable next step is to dig deeper. This is where you can move beyond simply screening and start truly measuring. A tool from Orange Neurosciences provides the objective data a questionnaire just can’t, especially for vague but debilitating symptoms like poor concentration or memory lapses.
By adding an AI-powered cognitive assessment to your process, you can transform a patient’s subjective complaint into a precise, actionable cognitive profile. In less than 30 minutes, you can get hard metrics on core functions, such as:
Attention: How well can they actually sustain their focus over time?
Memory: Are they struggling with short-term recall specifically?
Executive Function: What is their real capacity for planning and problem-solving?
Processing Speed: How quickly are they able to take in and respond to new information?
This two-pronged approach gives you the complete picture of your patient’s brain health: their emotional state from the PHQ-9, paired with their cognitive function from an objective assessment. It’s a powerful combination that allows you to build faster, better-informed, and far more effective treatment plans.
It's time to stop guessing and start measuring. When a PHQ-9 raises a red flag, you have a clear next step. Discover how to integrate AI-powered tools into your clinical workflow by exploring our complete guide to mental health assessment and contacting us for a demo.
Talking Through the PHQ-9: Your Common Questions Answered
When you start using the PHQ-9 in your daily practice, a few common questions always seem to pop up. Getting comfortable with these nuances is what separates a good screening process from a great one. Let's walk through some of the questions I hear most often from fellow clinicians.
How Often Should I Use the PHQ-9?
The simple answer is: it depends. Think of it like adjusting the focus on a camera—you need a sharper, more frequent look when the details really matter.
For a new patient or initial screening: A single administration gives you that crucial first baseline.
During active treatment: I've found that checking in every 4 to 6 weeks is the sweet spot. It’s frequent enough to see if your treatment plan is working but not so often that the patient gets tired of the questions. A 5-point drop in their score is a great sign that you're on the right track.
For "watchful waiting": If someone scores in that mild range (5-9) and you've decided to hold off on active treatment for now, a follow-up at their next appointment is a good idea. This helps you catch any changes, for better or worse.
So, Can the PHQ-9 Actually Diagnose Depression?
In short, no. The PHQ-9 is an incredibly valuable screening and monitoring tool, but it's not a diagnostic one. It’s brilliant at flagging individuals who are likely struggling with depression and helping us understand how severe their symptoms are. But a diagnosis? That's where your clinical expertise comes in.
A high PHQ-9 score is like a smoke alarm—it signals a potential fire, but it doesn't tell you the cause or the extent of the damage. A formal diagnosis requires your clinical judgment, a patient history, and a thorough assessment to rule out other causes.
What if the Score Is High, but My Patient Says They Aren't Depressed?
This happens all the time, and it's a pivotal moment. If a patient scores a 17 but insists, "I'm not depressed," your job isn't to correct them—it's to get curious. There are a few things that could be going on here.
They're feeling it physically. The patient might be experiencing their distress as purely physical. Look at their individual answers. Are the scores high for fatigue, sleep problems, and appetite changes? Frame the conversation around those tangible symptoms.
Stigma is a powerful force. The word "depression" can feel heavy and scary. A patient might be more open to talking about "burnout," "feeling overwhelmed," or "stress."
They just don't see the connection. Some people genuinely don't connect their individual symptoms to a larger pattern of depression.
Actionable Insight: Instead of asking, "Are you depressed?" shift your approach. Try something like, "I can see from your answers that you've been really struggling with energy and concentration lately. Can you tell me more about how that's been affecting your day?" This opens the door for a real conversation, without forcing a label they're not ready for.
When a PHQ-9 score points to a problem, take the next step. At Orange Neurosciences, we provide the objective, AI-powered cognitive assessments that turn subjective reports into precise data. Move beyond guessing and start measuring. Visit us at https://orangeneurosciences.ca or email us to learn how our tools can integrate into your practice and transform your patient outcomes.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation