Preschool Language Scales 5: Clinician's Guide 2026

A quiet 4-year-old is sitting on the clinic floor, turning a toy in his hands and glancing at his parent before every response. Daycare has raised concerns. The family isn't sure whether he's shy, overloaded, learning in more than one language, or missing key language milestones. That's where clinicians often reach for the Preschool Language Scales, Fifth Edition.
The PLS-5 remains one of the most familiar early-language tools in paediatric practice, but familiarity can create false confidence. A standard score isn't the diagnosis. A low score isn't self-explanatory. A child who doesn't say much in the room may still understand far more than the test captures, and a child who performs well in structured play may still struggle in daily life.
Used well, the PLS-5 helps organise clinical thinking. Used poorly, it can flatten a complex developmental picture into a single label. If you work in speech-language pathology, developmental paediatrics, psychology, early intervention, or school readiness screening, that distinction matters. For a broader view of how formal language testing fits within a full clinical workup, Orange Neurosciences' overview of speech-language pathology assessment is a useful companion read.
Navigating Early Language Assessment
The practical problem isn't identifying that a child seems delayed. It's deciding what the behaviour in front of you means.
A quiet preschooler can look language-impaired for several different reasons. He may have a genuine receptive or expressive language disorder. He may understand well but freeze in unfamiliar settings. He may be processing two languages and showing uneven performance across contexts. He may also have broader developmental differences affecting attention, play, regulation, or social communication.
What the referral question should sound like
Before you open the test kit, tighten the clinical question. “Does this child have a language delay?” is too broad to guide good testing. Better questions include:
Understanding concern: Is the child failing to understand spoken language, or only failing to show it during structured tasks?
Expression concern: Is spoken output limited across settings, or mostly in unfamiliar adult-led situations?
Context concern: Does performance change with parent support, home language, peer interaction, or play routine?
Decision concern: Are you screening for next steps, planning treatment, or informing eligibility?
Those questions shape how much weight you should give the PLS-5 result.
Many teams are also rethinking where standardised tools sit within earlier support pathways. That's one reason Soul Shoppe's early intervention insights are worth reading. They acknowledge that early concern rarely arrives as a neat diagnostic picture. It arrives as uncertainty, and children benefit when professionals respond before that uncertainty hardens into delay.
Clinical lens: The test helps most when you already know what decision you're trying to make.
What works in real practice
The PLS-5 is useful when you need a structured snapshot of early language across developmental levels. It works best when paired with observation, caregiver interview, and a clear understanding of why the child was referred.
What doesn't work is treating it as a stand-alone answer. If a child is fatigued, minimally verbal in unfamiliar settings, or navigating more than one language environment, the score may describe test performance more than underlying capacity.
What Is the Preschool Language Scales 5
The Preschool Language Scales, Fifth Edition functions like a developmental yardstick for early language. It's designed for children from birth through 7 years, 11 months and includes two core subtests, Auditory Comprehension and Expressive Communication, while also capturing pre-verbal interaction, vocabulary, concepts, language structure, and early literacy according to this PLS-5 overview.
That breadth is one reason clinicians keep coming back to it. You can use the same instrument family across a wide developmental span, rather than switching tools every time a child moves from infant services to preschool or from preschool into early school-age follow-up. If you want a refresher on how these domains unfold developmentally, Orange Neurosciences' discussion of language acquisition fits well beside the PLS-5 framework.
Why clinicians describe it as play-based
The PLS-5 doesn't feel like a desk test. That matters. Young children often reveal more in interaction than in direct questioning.
The tool uses activities, prompts, pictures, and objects to sample what the child understands and how the child communicates. For infants and very young toddlers, that may involve social attention, gesture, vocalisation, and early routines. For older children, the demands shift toward concepts, sentence-level understanding, verbal responses, and early literacy-related tasks.
What the two main parts tell you
The subtests answer different clinical questions:
Auditory Comprehension: What does the child understand from spoken language?
Expressive Communication: What can the child communicate through vocalisation, words, phrases, or more complex language?
Used together, they help you see whether the profile is balanced or uneven. A child may comprehend much more than they can express. Another may talk often but miss key concepts, relational terms, or grammatical information.
Don't think of the PLS-5 as “a speech test”. It samples language development from pre-verbal communication through early literacy-linked skills.
That broader scope is also why the PLS-5 often sits at the front end of decision-making. It can flag concern, organise strengths and weaknesses, and help determine whether you need deeper testing next.
Understanding the PLS-5 Subtests and Structure
Most interpretation errors start with a shallow understanding of what the two scales are measuring. If you only remember “receptive versus expressive,” you'll miss the developmental detail that makes the test clinically useful.
Auditory Comprehension in practice
Auditory Comprehension asks whether the child understands spoken language, but that understanding looks different at different developmental levels.
In very young children, you may be observing responses to voices, routines, social cues, and early word recognition. In preschoolers, the demands often involve following directions, identifying named objects or actions, and understanding concepts such as location, quantity, or comparison. In older children, items can place greater weight on sentence interpretation, more complex linguistic structures, and meaning embedded in broader language tasks.
A practical example helps. A younger child may be asked to identify a familiar object among choices. A preschooler might need to act on a direction such as placing one object in relation to another. An older child may need to interpret a longer spoken statement and respond accurately without visual guessing.
Expressive Communication in practice
Expressive Communication measures how the child sends language back into the interaction.
At the earliest level, this may involve vocal play, social reciprocity, or communicative intent rather than clear words. Later, the scale samples naming, requesting, commenting, combining words, using grammatical forms, and generating more organised spoken language.
Clinically, I pay close attention to how much support the child needs to respond. Some children can produce labels easily but struggle to explain, describe, or narrate. Others have scattered single words but use gesture, gaze, and play very effectively. The score may place them in a similar range, but the treatment plan should not look the same.
Quick-reference table for skill areas
Scale | Skills Assessed (with examples) |
|---|---|
Auditory Comprehension | Understanding names of common objects, following simple directions, interpreting basic concepts such as location or size, responding to more complex spoken language, showing understanding of early literacy-linked tasks |
Expressive Communication | Vocalising intentionally, using gesture with communication purpose, naming objects or actions, combining words, answering questions, describing pictures, explaining functions, producing more organised spoken language |
For a broader look at how language measures relate to other standardised learning tools, Orange Neurosciences' guide to individual achievement tests can help frame where the PLS-5 sits and where it doesn't.
What junior clinicians often miss
The most useful information often isn't the total result. It's the pattern within item performance.
Look for things like:
Strong object vocabulary with weak concept language
Good rote responses with poor novel sentence understanding
Adequate naming but limited generative language
Better non-verbal engagement than verbal output suggests
A sharp drop when auditory load increases
Those patterns tell you whether the issue is likely lexical, syntactic, processing-related, interactional, or tied to testing context.
A child who can point accurately but can't explain, retell, or answer open questions isn't simply “fine receptively and weak expressively”. That profile needs closer analysis.
Administering and Scoring the PLS-5
The difference between a useful PLS-5 administration and a messy one usually comes down to structure. The child should feel like they're playing, but the clinician still has to protect standardisation.
The PLS-5 is an individually administered, norm-referenced, play-based language assessment for children from birth to 7 years, 11 months. It yields standard scores, growth scores, language age equivalents, and percentile ranks, and that score set is designed for tracking change over time in early language intervention and monitoring, as summarised in this TxAUTISM description of the PLS-5. If you want a parallel discussion of why score stability matters, Orange Neurosciences also offers a plain-language guide to test-retest reliability.
Administration habits that improve test quality
A few habits matter more than people think:
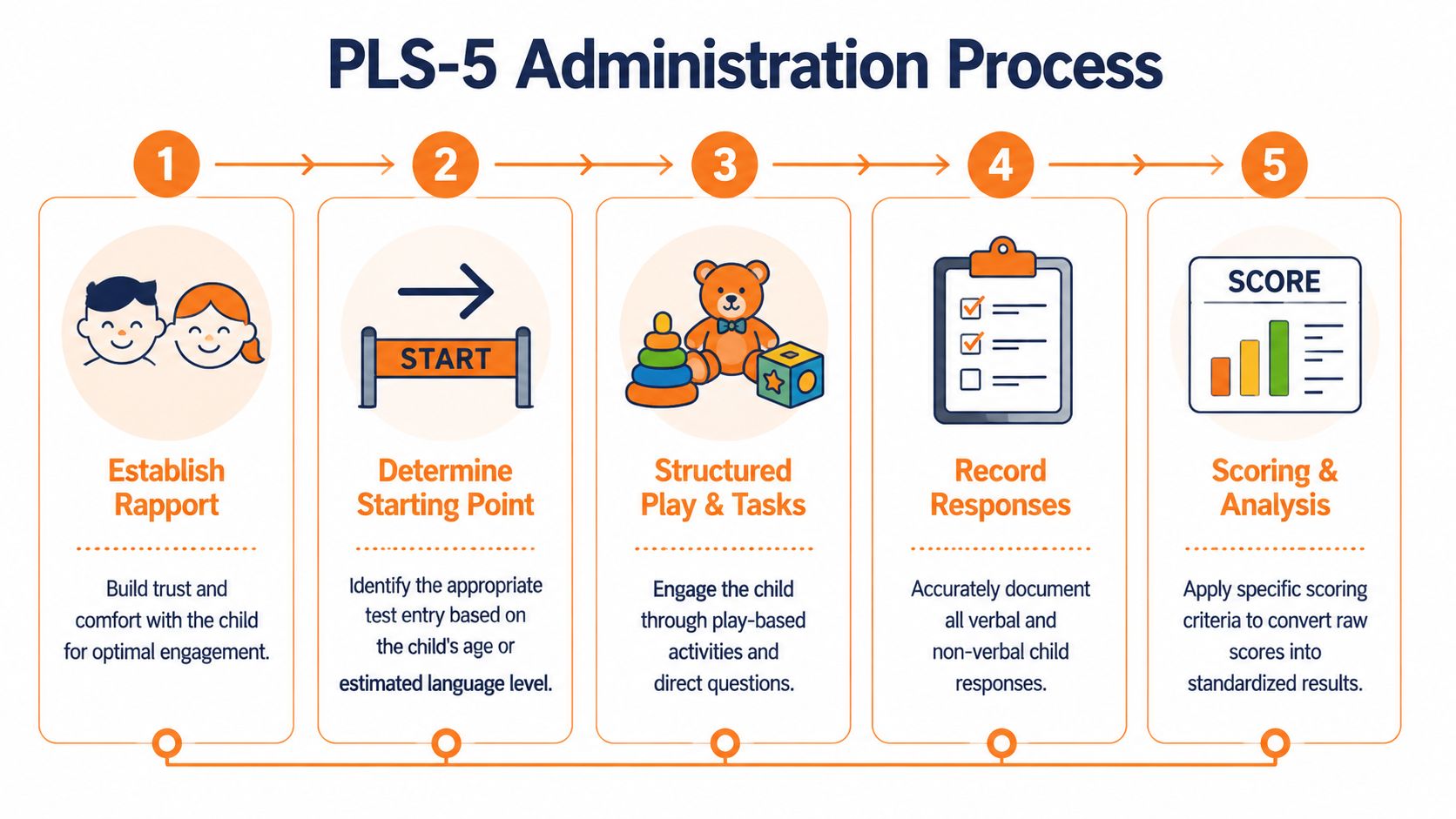
Set up before the child enters. If you're searching for materials mid-session, you lose attention and behavioural momentum.
Establish rapport quickly. Some children won't show true skill until they trust the routine.
Follow the test order carefully. Improvising can blur whether a response was spontaneous or cued.
Record in real time. Delayed scoring invites memory errors, especially with approximations or partial responses.
The play-based design helps, but it doesn't rescue poor pacing. If the child is drifting, reset with a clean transition rather than talking through the pause for too long.
Making sense of the score outputs
Different score types answer different questions:
Standard scores help compare a child's performance to the normative framework.
Percentile ranks can be useful for family discussion, but they're easy to over-interpret if you don't explain limitations.
Language age equivalents often make intuitive sense to parents, yet they can oversimplify uneven profiles.
Growth scores are especially helpful when you're monitoring change over time.
The mistake I see most often is over-relying on age equivalents because they sound concrete. They're not the best summary of clinical complexity. If a child has islands of strength and major gaps, age equivalents can make the profile sound flatter than it is.
What helps during difficult sessions
Use the materials as intended: The manipulatives and pictures are there to support engagement and consistency.
Protect response opportunities: Don't rescue too early. Silence is often where the child organises language.
Note behaviour beside the score: Attention shifts, refusal patterns, impulsive pointing, and parent dependence all affect interpretation.
Interpreting Results and Clinical Implications
A low PLS-5 score is a signal. It is not an explanation.
That point matters even more for children from low-SES and diverse language backgrounds, where independent research has raised concerns about how trustworthy PLS-5 scores are in those populations and whether the instrument should be used for eligibility decisions without supplemental data, as discussed in this PubMed-indexed psychometric analysis.

Case pattern one with uneven scores
A child shows relatively stronger Auditory Comprehension than Expressive Communication. In the room, he follows familiar directions, identifies named items, and responds non-verbally with clear intent. Spoken output is sparse. He whispers to his parent, avoids direct verbal response, and produces less language with the examiner than at home.
A profile like this can point toward expressive language weakness. It can also reflect performance factors such as anxiety, selective speaking patterns, unfamiliar examiner interaction, or high demand for verbal output. If you stop at “expressive delay,” you may miss the actual barrier.
What helps next:
Language sampling across contexts
Parent and educator report
Observation of peer interaction
If relevant, mental health or behavioural follow-up
Case pattern two with globally low scores
Another child scores low across both scales. During administration, you also see limited symbolic play, inconsistent attention to task, reduced social reciprocity, and difficulty learning from prompts.
That pattern may reflect a broader developmental issue rather than an isolated language disorder. The PLS-5 can flag that concern, but it can't tell you whether the underlying driver is global developmental delay, autism-related communication differences, regulation difficulty, hearing-related concerns, or something else.
Interpretation rule: Always ask whether the score reflects language knowledge, test access, or both.
Where clinicians need the most caution
The hardest cases are often children in dual-language environments, children who use non-mainstream dialects, or children whose daily communication looks stronger at home than in the clinic. In those cases, a low score should prompt more questions, not more certainty.
Useful follow-up options include:
Bilingual assessment: Necessary when the child's language exposure and use aren't well represented by the testing context.
Language sample analysis: Often reveals communicative strengths that item-level testing misses.
Dynamic assessment: Helpful when you need to know how the child learns with support.
Caregiver interview: Essential for separating limited test-room performance from daily communicative ability.
What doesn't work is using one low norm-referenced score as stand-alone proof of disorder. That approach increases the risk of misclassification, especially where language difference may be mistaken for impairment.
The PLS-5 in Modern Practice and Its Complements
The PLS-5 still fits modern practice, but not because it does everything. It fits because it does one job reasonably well: it samples early language across a broad developmental range in a structured, child-friendly format.
Recent updates added items for letter naming, book handling, and school-readiness skills, which has made the measure more relevant for preschool programmes. At the same time, clinicians still need supplemental measures like caregiver reports and broader cognitive screens to understand why a child earned a given score and to reduce misclassification risk, as noted in Reach Out and Read's PLS metric summary. For readers comparing language testing with broader neurodevelopmental methods, Orange Neurosciences' overview of cognitive assessment tools provides a helpful contrast.
Where the PLS-5 ends
Language performance depends on more than language knowledge. A child may miss items because of attention drift, working memory limits, processing inefficiency, poor task persistence, or weak tolerance for adult-led demand. The PLS-5 can show you the behavioural effect of those issues, but it isn't built to isolate them.
That distinction changes treatment planning. If a child's expressive performance collapses when auditory load rises, you may be looking at more than an expressive language problem. If a child misses comprehension items inconsistently, attentional control may be part of the picture.
What a modern assessment battery should include
In current practice, strong assessment usually combines:
Standardised language testing: To capture formal performance in receptive and expressive domains
Functional observation: To see how language works in play, transition, and interaction
Caregiver information: To anchor interpretation in real-world communication
Broader developmental or cognitive data: To understand what may be driving the language profile
That integrated model is more defensible than relying on the PLS-5 alone. It also produces better goals. Instead of writing “improve expressive language,” you can target the actual bottleneck, such as concept vocabulary, sentence formulation, verbal initiation, or comprehension under increased processing demand.
Frequently Asked Questions About the PLS-5
Who can administer the PLS-5
Use the PLS-5 within your scope, training, and local professional standards. In practice, that usually means speech-language pathologists and other qualified professionals who've been trained to administer standardised developmental measures properly. If someone doesn't understand basal and ceiling logic, standardised prompting limits, or score interpretation, they shouldn't be giving the test independently.
How does the PLS-5 compare with the CELF-P
They answer related but not identical clinical needs. The PLS-5 is often more useful for younger children, children with emerging communication, and children who need a more interactive, play-based format. The CELF-P can be helpful when you need a more detailed look at language structure in a child who can tolerate more formal verbal tasks.
A simple rule works well in practice:
Choose the PLS-5 when developmental range, play-based access, and early language sampling matter most.
Choose the CELF-P when you need a more explicit breakdown of language form in a child who can manage that testing style.
When should you re-administer it
Reassessment should match the clinical question. If you're monitoring intervention, wait long enough for meaningful change to occur and avoid re-testing so quickly that familiarity drives performance. If the issue is diagnostic uncertainty rather than progress monitoring, use follow-up tools or contextual measures first when they're more likely to answer the unresolved question.
When the first administration leaves you unsure whether you measured language ability or test-room behaviour, repeating the same test isn't always the best next step.
If you're building a more complete assessment pathway, Orange Neurosciences can help add rapid, objective cognitive profiling alongside your language work. Their platform supports clinicians who need clearer data on attention, memory, executive function, processing speed, perception, and related domains so referral decisions and intervention plans don't rely on guesswork alone.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation