Acquisition of Language

A two-year-old in clinic pointed to the snack shelf, paused, and said, “more crackers”. Her mother smiled because it sounded simple. Every clinician in the room knew it wasn't simple at all.
Those two words carried listening, memory, motor planning, social intent, and a growing ability to map sound to meaning. That is the everyday wonder behind the acquisition of language.
The Miracle of Our First Words
A child's first words often look like tiny events. In reality, they're the visible tip of a much larger developmental process. Before a toddler says “up”, “mama”, or “all gone”, the child has already spent months sorting speech sounds, noticing patterns, linking words to routines, and learning that communication changes what other people do.

Language starts before words appear
Parents sometimes worry when they don't hear many words yet. That concern is understandable, but speech is only one part of language development. Long before expressive language becomes obvious, babies are building receptive systems. They learn turn-taking through face-to-face play. They begin to predict routines. They hear that some sound patterns belong together and others don't.
A practical example helps. If a baby hears “Where's your shoe?” during dressing every day, the baby isn't memorising a school-style lesson. The child is gradually connecting sounds, objects, actions, and expectations. Language grows through repeated exposure embedded in real life.
One reason this matters so much in Canada is that many children hear more than one language from the start. The 2021 Census context on multilingual mother tongue use notes that 9.6 million people in Canada reported a mother tongue other than English or French, representing 25.4% of the population. It also notes that 7.8 million people, or 21.4%, reported speaking a language other than English or French most often at home. For clinicians and educators, that means language acquisition is often happening across multiple speakers, settings, and sound systems.
Practical rule: When a child is exposed to two or more languages, ask about total communication across settings, not just one language in one room.
Why first words matter beyond vocabulary
First words are not only labels. They mark a shift in how a child participates in learning, attachment, and self-regulation. A child who can say “help”, point to “ball”, or understand “give it to Nana” is building tools for classroom participation and social problem-solving.
That's also why milestone guides can be useful when families need a simple starting point. A plain-language baby speech milestones guide can help parents notice what comes before fluent talking and when to seek a closer look.
A classic finding often used to illustrate how rapidly language grows is that children learn 10 to 15 new word meanings per day, with only about 1 of those tied to direct teaching. The bigger lesson isn't the number alone. It's that children learn language mostly from immersion in meaningful interaction, not from formal instruction.
What clinicians and educators should listen for
When I observe a young child, I'm not waiting only for a word list. I'm listening for a broader pattern:
Attention to speech: Does the child orient to voices, songs, and name calls?
Shared routines: Does the child anticipate familiar phrases during meals, books, or play?
Intent to communicate: Does the child point, gesture, vocalise, or seek a response?
Flexibility across people: Does communication change with parents, siblings, educators, or peers?
Those early signs tell us whether the system underneath language is organising well. Words come out of that system. They don't appear in isolation.
How We Learn to Talk Major Theories Explained
If you've ever sat through a language development lecture and thought, “These theories seem to disagree about everything,” that reaction makes sense. Each theory focuses on a different piece of the same puzzle. I often explain them to educators as four different ways of describing how a house gets built. One emphasises the tools, another the blueprint, another the people in the room, and another the repeated patterns in the materials.
Four useful lenses, not four enemy camps
Theories of language acquisition are most helpful when we treat them as working lenses.
Theory | Core Idea | Mechanism | Example |
|---|---|---|---|
Behaviourist | Children learn language through imitation and reinforcement | Adults model words, children repeat them, useful attempts are reinforced | A child says “juice”, and the adult responds by giving juice and praising the request |
Nativist | Children are biologically prepared for language | Inborn capacities help children detect grammar and organise input | A child produces a sentence pattern they were never directly taught |
Social-interactionist | Language grows through human interaction | Joint attention, turn-taking, and responsive communication drive learning | A caregiver follows the child's focus and labels what the child is looking at |
Usage-based | Children build language from patterns in what they hear | Repeated exposure helps the child detect regularities and form constructions | A child hears “want more”, “want up”, and “want juice”, then begins using similar frames |
Behaviourist ideas remind us that feedback matters. If a child says “ball” and an adult responds warmly, that exchange increases the value of communication. But behaviourism alone doesn't explain how children produce sentences they've never copied word for word.
Nativist theories help explain why language learning seems to unfold so powerfully in young children. Yet a purely innate explanation can make clinicians underestimate the importance of environment, interaction, and access.
Social-interactionist models fix that problem. They emphasise that children learn language with people, not around people. A screen can expose a child to words, but responsive back-and-forth interaction does much more developmental work.
Usage-based approaches have become especially practical for educators because they align closely with what we observe in real classrooms. Children hear patterns repeatedly, begin to detect structure, and gradually generalise.
The evidence that changed the conversation
One major turning point came when research showed that 8-month-old infants can track the statistical structure of speech to find word boundaries. That finding, discussed in this review of statistical learning in language development, helped move the field beyond a simple “rules versus imitation” debate.
That matters in practice. It means infants don't need perfectly separated words to begin learning. They can use probability and pattern. If one set of sounds often occurs together, the infant starts treating it as a unit.
A useful clinical analogy is this: children are not just storing words like flashcards. They're acting more like pattern detectors in a noisy environment.
For many clinicians, this also helps explain why some children seem to know more than they can say. The internal system may be learning from exposure before expressive output catches up.
Why theory matters for assessment
Assessment gets sharper when we know what each theory highlights. If you lean only on milestones, you may miss the child who has weak social reciprocity. If you focus only on interaction, you may miss the child whose attention or processing constraints interfere with language uptake. If you care only about vocabulary counts, you may overlook pattern learning.
That's why I often encourage teams to connect language observations with broader thinking skills such as memory, attention, and processing efficiency. This overview of cognitive function in learning and daily performance is a useful companion for that discussion, especially when a child's language profile doesn't fit a simple delay model.
In other words, theory is not an academic extra. It changes what we notice, what we measure, and how we intervene.
From Coos to Conversation Key Developmental Milestones
Milestones help because they turn an invisible process into observable behaviour. They also create a common language for families, educators, and clinicians. The problem is that milestone lists are often read too rigidly. They should guide professional judgement, not replace it.

What early development often looks like
In the earliest months, children usually communicate through voice quality, crying patterns, gaze, and body movement. Cooing and babbling matter because they show the child is practising sound production and social timing.
By the end of the first year, many children begin using first words in context. These words are often tied to daily routines and highly meaningful people or objects. “Dada”, “bye”, “up”, and “no” are common because they are functional.
Between the second year and the preschool period, language becomes combinatorial. Children begin to join words, then build simple sentences, then tell short narratives.
A practical timeline for observation
Birth to 6 months: Listen for cooing, vocal play, response to voices, and early turn-taking in sound.
6 to 12 months: Look for babbling with varied sounds, response to name, and first meaningful word attempts.
12 to 24 months: Watch for single words expanding into two-word phrases such as “more milk” or “Daddy go”.
2 to 3 years: Expect simple sentences, growing vocabulary, and better understanding of directions in routine contexts.
3 to 5 years: Notice longer conversations, question forms, storytelling attempts, and language used for pretend play and peer interaction.
A practical example from nursery settings: a two-year-old who says “truck go” is doing more than combining two words. The child is showing early syntax, event representation, and the ability to compress meaning efficiently.
When families say, “She understands everything but doesn't talk much,” ask what “everything” means. Understanding familiar routines is not the same as understanding language across new contexts.
Milestones in multilingual and second-language contexts
Many teams often face a challenge. A child learning more than one language may distribute skills across languages rather than showing the same vocabulary in each. That can make a child look weaker if we assess only one language in isolation.
For older learners acquiring an additional language at school, progress should also be interpreted realistically. The overview of second-language acquisition timelines notes that learners with strong first-language literacy often need 5–7 years to reach advanced fluency, and that the timeline can extend to 7–10 years if first-language literacy is underdeveloped.
That single point protects many children from unfair expectations. A newcomer student who can participate socially but still struggles with academic language may be following a normal long-range acquisition pathway rather than showing a disorder.
When milestones help most
Milestones are most useful when they trigger better questions, such as:
Across settings: Does the child communicate differently at home, daycare, and school?
Across modalities: Is the child using gestures, signs, pictures, or spoken words?
Across demands: Can the child understand routine language only, or also new directions and decontextualised talk?
Those questions move us from checklist thinking to clinical reasoning.
The Brains Blueprint for Language
Language feels effortless when it's working well. Underneath, it depends on multiple brain systems coordinating at speed. I explain this to families with a factory analogy. One system helps decode incoming sound, another helps organise meaning, another plans speech, and another carries out the movements needed to speak clearly.
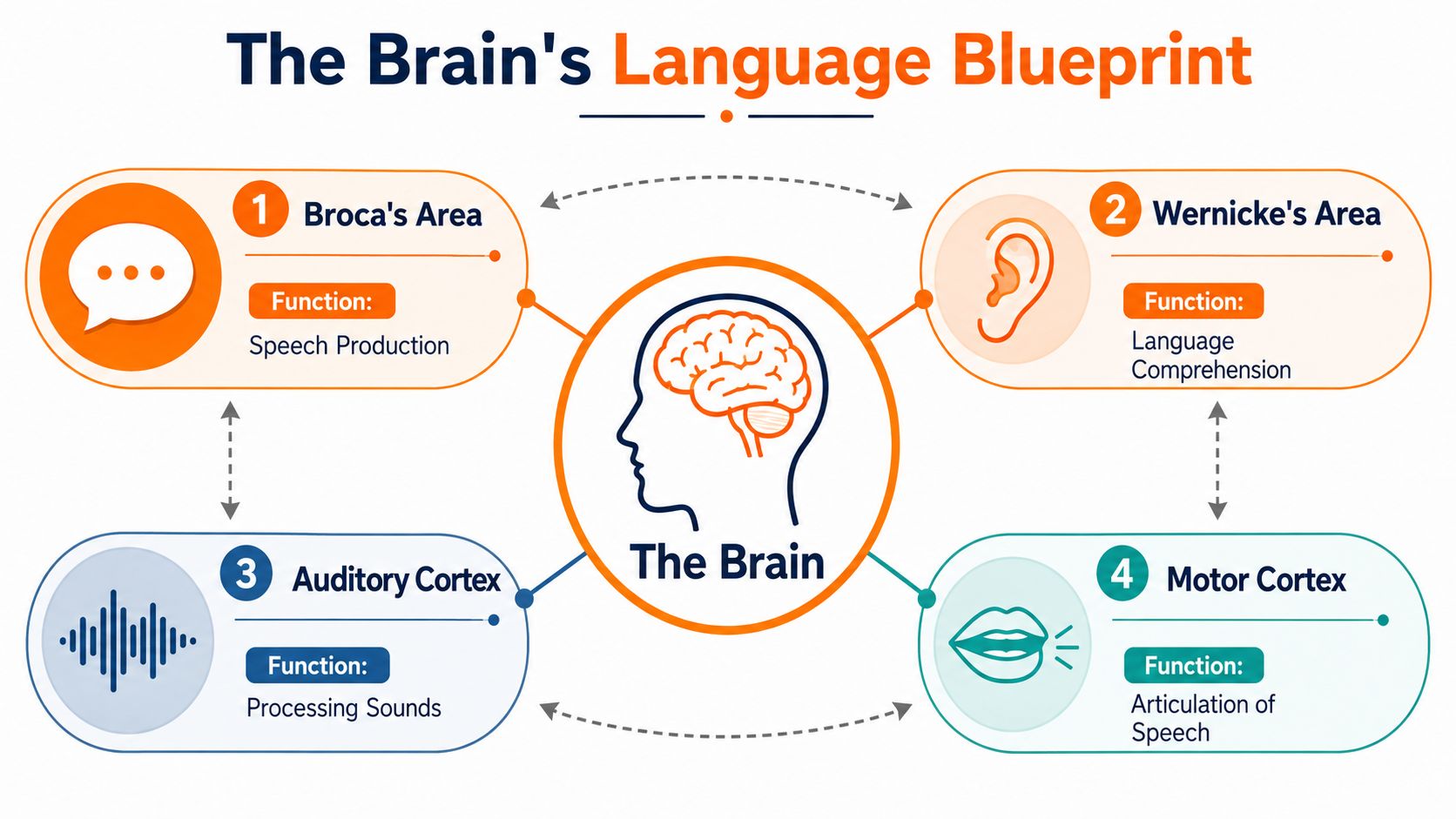
What the brain has to do during language
A child hearing “Put the red cup on the table” must process sound, separate words, hold the sequence in working memory, connect words to meaning, inhibit distractions, and plan a response. If any part of that chain is strained, language performance can look uneven.
This is why language problems don't always begin with language alone. Attention, auditory processing, working memory, and motor planning all shape how well a child can acquire and use language.
For clinicians who want a quick refresher on brain organisation, this guide to the lobes of the brain and their functions is a helpful reference when explaining why communication depends on distributed systems rather than one isolated “language centre”.
Why early exposure matters so much
The brain is especially responsive to language early in life. Researchers often describe this in terms of plasticity. In plain language, the developing brain is more ready to tune itself to the sound patterns and grammatical structures it hears regularly.
A large-scale analysis summarised in this critical period research review supports a sharply defined critical period for grammar acquisition, with performance declining when second-language learning begins later in life. For practice, the takeaway is not that later learning is hopeless. It isn't. The takeaway is that age changes how learning happens.
Young children tend to absorb structure more implicitly. Older learners often rely more on explicit strategies, conscious study, and accumulated practice.
What this means for intervention
If the brain is most malleable early, then waiting for a child to “grow out of it” can cost valuable time. That doesn't mean every variation is a disorder. It means persistent concerns deserve timely screening.
Early support works best when it matches the child's developmental stage, not when it copies goals designed for older children.
In schools and clinics, that principle affects everything from referral timing to therapy targets. A preschooler with limited understanding needs rich, repeated, interactive input. An older student may also need metalinguistic support, literacy scaffolding, and strategies that reduce memory load.
The brain's blueprint doesn't tell us everything. But it does tell us this: language intervention is not just educational. It is developmental timing in action.
Screening for Language Delays and Differences
The hardest part of language support is often the first decision. Is this child showing a normal variation, a difference related to multilingual exposure, or a delay that needs formal follow-up? Many referrals happen because adults notice something is off but can't yet describe the pattern clearly.

What traditional screening does well
Parent report, teacher observations, play-based interaction, and direct speech-language assessment remain essential. They capture context. They show how the child communicates with familiar people. They reveal whether language breaks down during transitions, peer interaction, or classroom demands.
A skilled speech-language pathologist can learn a great deal from spontaneous language sampling and structured observation. This overview of a speech-language pathology assessment process is useful for teams who want a practical sense of how referral questions become a more organised evaluation plan.
Where confusion often starts
Observation has limits. Parents may compare a child to a sibling rather than to developmental expectations. Teachers may see the child only in one language or one setting. A bright child may compensate socially and mask comprehension difficulty. Another child may say very little in clinic but communicate well at home.
This is also why language concerns often overlap with reading concerns. If a child struggles to hold meaning across sentences, follow oral directions, or retrieve vocabulary efficiently, those same underlying issues may later affect literacy. Families trying to connect spoken language and comprehension may find this article on understanding child's reading difficulties helpful as a practical companion.
Why objective profiling matters
When language is weak, professionals often ask, “Is this really a language issue?” That question is too broad. A more useful question is, “Which underlying processes are helping or constraining language performance?”
Consider two children with similar expressive delays:
Child A understands well but struggles to retrieve words quickly.
Child B has difficulty sustaining attention long enough to encode verbal input.
Child C hears and imitates words but breaks down when tasks require working memory.
Child D speaks little because the language of instruction is not the strongest language used at home.
All four may look similar in a brief conversation. They do not need the same intervention.
Good screening narrows uncertainty. It doesn't just label the surface behaviour.
That's where objective cognitive indicators become useful. Measures related to attention, processing speed, memory, and executive control can help teams interpret language performance more accurately. They don't replace clinical judgement. They strengthen it by reducing guesswork.
For educators and clinicians, the gain is primarily practical. Better profiling leads to better decisions about referral urgency, classroom accommodations, and whether a child needs language therapy, literacy support, broader neurodevelopmental evaluation, or a combination.
Practical Strategies for Personalized Language Support
One-size-fits-all language support usually fails for a simple reason. The same outward symptom can come from very different underlying needs. “Late talking” can reflect limited exposure, weak comprehension, reduced interaction, hearing-related access issues, broader cognitive strain, or a combination.
Match support to the barrier
A child who doesn't understand enough language input needs a different plan from a child who understands but can't organise an output. That sounds obvious, but many interventions still rely on generic vocabulary drilling.
In real settings, the most effective supports are usually specific and modest. A preschool educator might reduce sentence length, pause after key words, and repeat a phrase in the same routine over several days. A clinician might target turn-taking and joint attention before pushing for longer expressive output. A classroom teacher might pre-teach key concepts visually before introducing a new topic discussion.
Accessible language matters more than modality debates
One of the most overlooked areas in discussions of the acquisition of language is support for deaf and hard-of-hearing children. The primary issue is not hearing status by itself. It is access to early, rich, accessible language.
The review on language deprivation and accessible input in deaf and hard-of-hearing children makes this point clearly. Natural sign languages are acquired on the same timeline as spoken languages when fluent input is available from birth. That changes the practical question. Instead of asking whether speech or sign is universally “best”, clinicians and families need to ask whether the child can fully access language now.
A child with accessible signed input is not “waiting for language”. That child is acquiring language.
What works in multilingual classrooms
Canadian classrooms often include children learning English or French alongside one or more home languages. In that setting, strong support usually looks less like correction and more like design.
Try approaches such as:
Build comprehensible routines: Reuse classroom phrases during transitions, clean-up, and group time so children can predict language in context.
Use visual anchors: Pair oral language with gestures, objects, icons, and demonstration.
Protect the home language: Encourage families to keep speaking the language they use most comfortably and richly.
Create interaction, not just exposure: Children need chances to ask, answer, repair, and negotiate meaning.
For older independent learners, some of the same principles apply. This guide to Gaeilgeoir AI tips for solo language acquisition is aimed at self-directed learners, but its emphasis on consistent exposure and meaningful use mirrors what we know about language growth more broadly.
Personalisation needs service pathways too
Support doesn't happen only in therapy sessions. It depends on referral quality, family coaching, classroom follow-through, and realistic goal-setting. In Canada, many families also need help understanding what services involve. This overview of speech therapy in Canada is a practical resource for teams explaining next steps after a concern is identified.
Personalised support means choosing targets that fit the child's profile, the child's language environment, and the child's access needs. It also means defining success correctly. For one child, success may be more spoken words. For another, it may be stronger comprehension, more effective signing, better classroom participation, or fewer communication breakdowns during daily routines.
The Future of Language Support Is Objective Cognitive Profiling
Classic language theories gave us valuable explanations. Developmental milestones gave us observable markers. Neuroscience showed why timing matters. Clinical practice taught us that surface symptoms can be misleading.
The next step is to connect those insights with better measurement.
Observation is necessary, but it isn't enough
A teacher may report, “He doesn't seem to follow oral instructions.” A parent may say, “She talks at home but shuts down at school.” A clinician may hear reduced sentence length during assessment. All of those observations matter. None of them, on their own, tell us whether the main bottleneck is attention, processing speed, working memory, executive control, language access, or a combination.
Objective cognitive profiling helps fill that gap. Instead of relying only on impressions, teams can gather structured information about the underlying skills that support language learning and language use.
Where technology fits in
Tools such as Orange Neurosciences can be clinically useful. The platform provides objective cognitive profiles across areas such as attention, memory, executive function, perception, processing speed, and eye-hand coordination. In a language-support context, that kind of profile can help teams interpret why a child is struggling and whether the pattern points toward language intervention, broader cognitive follow-up, or both.
The guide on language of assessment in cognitive and educational evaluation is especially relevant here because assessment results only become meaningful when we interpret them in the right linguistic context.
The practical goal is not to replace the clinician or educator. It is to give them cleaner signals before they make high-stakes decisions.
Better profiles lead to better plans
When teams understand the cognitive profile behind language performance, intervention becomes more precise. Goals can be narrowed. Accommodations can be chosen with more confidence. Progress can be monitored against the right domain, rather than against vague expectations.
That matters for multilingual children, for children with suspected developmental language concerns, for deaf and hard-of-hearing children, and for students whose reading and language challenges overlap. In each case, the question is the same. What does this learner need in order to access language more effectively?
The acquisition of language is one of the most human processes we ever study. It deserves assessment methods that are just as thoughtful.
If you're trying to make language screening and intervention more precise, visit Orange Neurosciences to explore how objective cognitive profiling can support referral decisions, educational planning, and more personalised care. You can also contact the team directly through the website if you want to discuss how these tools may fit your clinic, school, or research setting.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation