A Guide to Speech Language Pathology Assessment

You might be here because something feels off, but you can't yet name it.
A parent notices their toddler understands routines but says very few words. A teacher sees a student who's bright in class discussion yet struggles to explain ideas clearly. An adult starts searching for words after a concussion, stroke, or other neurological change and wonders whether this is temporary or something that needs professional help.
That uncertainty is exactly why a speech language pathology assessment matters. It turns a vague worry into a structured clinical question. Beyond this, it helps families and clinicians move from guessing to understanding.
Understanding When a Communication Assessment Is Needed
A communication assessment is usually needed when everyday life starts showing a pattern. Maybe a child isn't combining words, can't follow directions expected for their age, or becomes frustrated because others don't understand them. Maybe an adult speaks clearly some days but loses track of conversations, forgets key words, or has trouble swallowing safely.

A speech-language pathologist (SLP) is trained to assess communication across speech, language, voice, fluency, cognition, and often swallowing. In schools, clinics, hospitals, and private practice, SLPs help answer questions like: Is this a delay, a disorder, a difference, or a skill that needs support?
California families often have access to school-based and medical routes for evaluation because the profession is well established. The U.S. Bureau of Labor Statistics reports that California employed 11,190 speech-language pathologists in May 2024, the highest state total in the nation, and BLS projects national employment to grow 15% from 2024 to 2034, with about 13,300 openings per year on average (speech-language pathologist employment outlook).
Common moments that prompt a referral
Speech is hard to understand even for familiar listeners.
Language isn't developing as expected, such as trouble understanding questions or putting words together.
School performance drops because listening, speaking, reading, or following directions is difficult.
Communication changes suddenly after a neurological event or injury.
Feeding or oral concerns appear, especially in infants or young children. If you're sorting through related oral-motor questions, resources from Charlotte infant tongue tie experts can help families understand one possible factor to discuss with a clinician.
Many parents wait because they hope a child will “catch up.” Sometimes that happens. Sometimes it doesn't. Assessment gives you a clearer basis for that decision.
If you're a new clinician, this is the first mindset to hold onto. Referral isn't a verdict. It's a request for clarity.
What a Speech Language Pathology Assessment Involves
People often picture assessment as a single test booklet and a final score. That's not how good clinical assessment works.
A speech language pathology assessment is closer to detective work. The SLP gathers clues from different places, checks whether they match, and asks what those clues mean in real life. A child who misses items on a vocabulary test may be struggling with attention, hearing, language exposure, task comprehension, or anxiety. A single score can't answer that by itself.
The real purpose of the assessment
An assessment usually aims to answer four practical questions:
What are this person's communication strengths?
What areas are difficult, inconsistent, or delayed?
Do the findings fit a clinical pattern or diagnosis?
What support should happen next?
That last question matters most to families. The assessment isn't just about labels. It's about decisions.
Why the process uses more than one tool
In school settings, the process is shaped by federal special-education requirements. IDEA requires evaluations to use a variety of technically sound assessment tools and strategies, to be non-discriminatory, and to be conducted in the child's native language when appropriate, as outlined in ASHA's school assessment guidance (ASHA guidance on school-based speech and language assessment).
That protects against a common mistake. If a clinician relies on one narrow test, they may confuse limited test performance with a true disorder.
What families usually experience
A typical assessment process may include:
A pre-assessment conversation about concerns, history, and goals
Direct testing or structured tasks to sample specific skills
Observation during conversation, play, classroom participation, or daily routines
Review of records such as teacher notes, medical reports, or previous evaluations
A feedback meeting where results are translated into plain language
Practical rule: If the clinician can't explain why they chose a task, or how the result connects to everyday communication, the assessment is probably too narrow.
For a worried parent, this means the process should feel purposeful, not random. For a new clinician, it means every tool needs a clinical reason behind it.
The Core Components of a Comprehensive Evaluation
The strongest evaluations are built like a layered picture. Each piece adds detail, and no single piece should carry the entire decision.
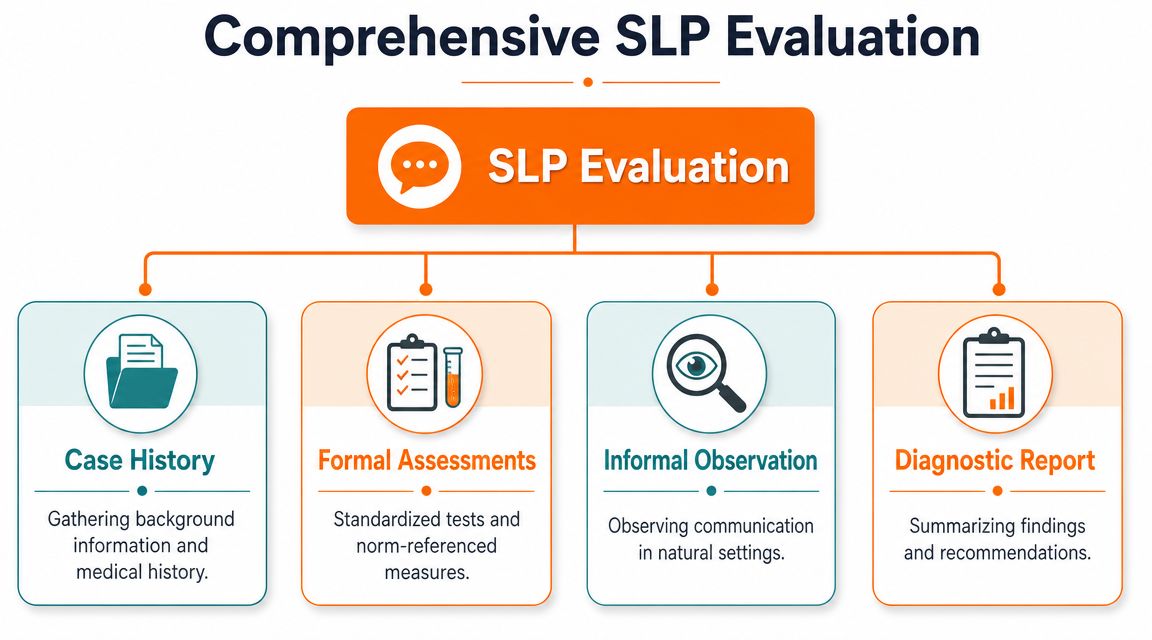
ASHA's practice patterns call for integrating case history, interviews, standardized and nonstandardized measures, speech samples, and functional observation, because a single score can miss the functional impact of a communication problem (ASHA practice patterns for speech-language assessment).
Case history gives context
The initial phase of assessment involves information gathering. The clinician asks about development, medical background, school performance, family concerns, and what the person can already do.
A few examples:
When did you first notice the stutter?
Which languages are spoken at home?
Has there been a hearing test?
What happens when your child gets stuck trying to communicate?
What changed after the injury?
Case history often explains why a test result looks the way it does. Without context, interpretation gets shaky.
Formal tests show performance under structured conditions
Standardized tests compare a person's performance to a reference group. They can be useful when the tool matches the person being assessed and the clinician understands the limits of the norms.
Think of these tests like taking blood pressure in a clinic. The result matters, but no good doctor would judge overall health from that one number alone.
If you work across disciplines, that logic is similar to understanding comprehensive eye exams. An eye exam doesn't stop at one reading. It combines different measures to understand function more accurately.
Informal measures show how communication works in the wild
Informal assessment often tells me more about daily function than a neat score ever could.
That may include:
Language samples during play or conversation
Speech samples to analyse sound errors
Classroom or workplace observation
Narrative tasks such as retelling a story
Dynamic support, where the clinician checks how performance changes with cues
A child might score modestly on a formal task but tell a rich story with visual support. An adult might perform well on short naming items yet struggle in longer, real conversations.
Diagnostic reporting pulls the pieces together
The report is not supposed to be a data dump. It should answer the referral question in a way families and teams can use.
Component | What it adds | Why it matters |
|---|---|---|
Case history | Background and timeline | Shows how concerns developed |
Formal assessment | Structured comparison data | Helps identify patterns |
Informal observation | Functional communication evidence | Shows real-world impact |
Diagnostic report | Clinical synthesis | Guides eligibility, treatment, and follow-up |
If you're new to clinical language, Orange Neurosciences has a useful guide on the language of assessment, especially for understanding terms that often confuse families and newer practitioners.
A good evaluation doesn't ask, “What score did we get?” It asks, “What does this mean for communication in daily life?”
Key Areas Evaluated During an Assessment
An SLP doesn't assess “speech” as one big single skill. Communication has separate parts, and each part can break down in a different way.
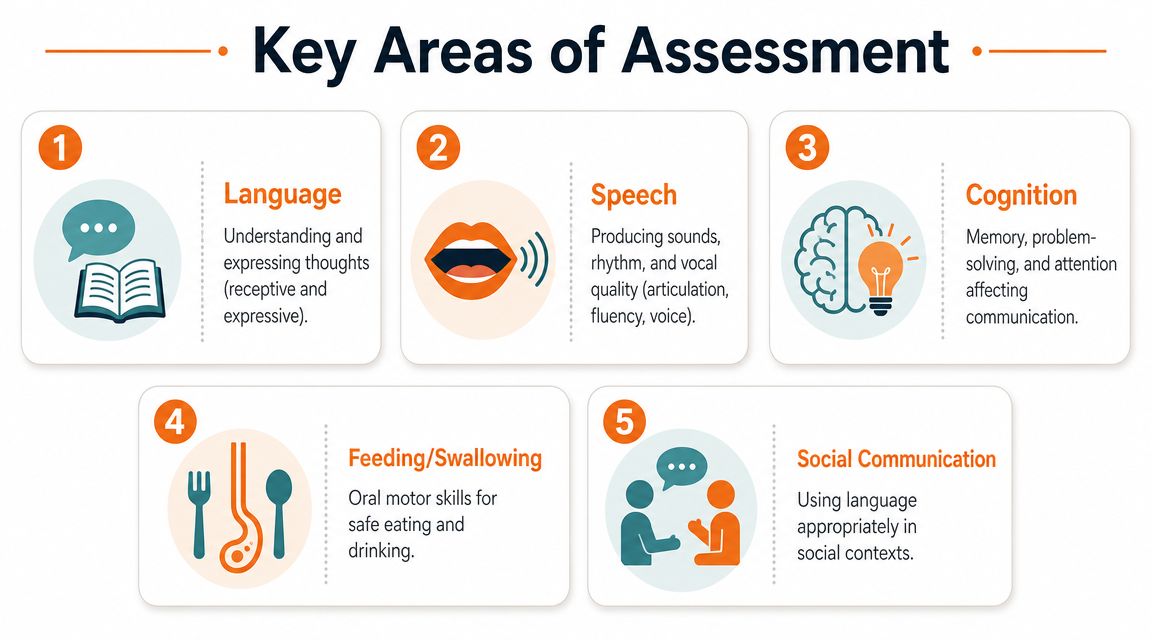
Speech and sound production
This area looks at how sounds are produced and organised.
Articulation is about individual sounds. A child may say “wabbit” for “rabbit.”
Phonology is about sound patterns. A child may leave off ending sounds across many words, not just one.
The distinction matters. One sound error calls for a different treatment plan than a broad phonological pattern.
Language
Language includes both understanding and using words, sentences, and meaning.
A child with receptive language difficulty may seem inattentive, when the deeper issue is that they don't fully understand multi-step directions. An adult with expressive language difficulty may know what they want to say but can't organise the words fast enough to say it.
Clinicians often look at:
Vocabulary knowledge
Sentence structure
Following directions
Storytelling and explanation
Word finding
If auditory processing questions are part of the picture, Orange Neurosciences also provides a practical overview of the auditory processing test and how it differs from broader language assessment.
Fluency, voice, and social communication
Not every referral is about pronunciation or language delay.
Fluency assessment looks at stuttering or other disruptions in the flow of speech.
Voice assessment considers pitch, loudness, quality, and vocal effort.
Pragmatics, or social communication, looks at how a person starts conversations, takes turns, reads social cues, and adjusts language to the situation.
A student may have strong vocabulary but struggle to stay on topic, read facial expressions, or repair misunderstandings. That's a different clinical picture from a child who mispronounces sounds.
Cognition and swallowing
Communication depends on brain skills like attention, memory, organisation, and processing speed. This is often called cognitive-communication. Adults with neurological conditions commonly show difficulties here, but children can too.
Some SLPs also assess feeding and swallowing, depending on setting and training. Oral-motor patterns, chewing, safe swallowing, and related muscle function may become part of the evaluation. Families exploring the broader oral-function picture sometimes benefit from learning what myofunctional therapy treats, especially when speech, breathing, and oral habits overlap.
When parents say, “My child talks, so why would language be a concern?” they're usually mixing up speech with language. Speech is the sound. Language is the system behind the message.
Pediatric Versus Adult Assessment Considerations
Children and adults may go through similar assessment components, but the clinical questions are very different.

With children, the question is often developmental. Is this skill emerging more slowly than expected, developing differently, or being affected by another factor such as hearing, attention, or language exposure? With adults, the question is often functional. What changed, why did it change, and how is it affecting independence?
What matters most in paediatric assessment
For children, assessment often needs to fit into play, classroom routines, and family life. A very young child may reveal far more in a play-based interaction than in a highly structured task.
Paediatric assessment usually pays close attention to:
Developmental expectations across communication areas
Learning impact in school or early education
Family routines and concerns
Peer interaction and behaviour regulation
Response to support, modelling, and cues
For multilingual children, this becomes even more important. Best practice is to examine speech in each language and consider dialectal variation, because using a standardized test based only on monolingual norms can be invalid and may lead to misdiagnosis (multilingual speech assessment guidance).
A child who mixes languages is not automatically showing disorder. A child who uses a dialectal pattern is not automatically making errors. The clinician has to know the difference.
What shifts in adult assessment
Adult assessment often follows an acquired change. Stroke, traumatic brain injury, progressive neurological disease, and other medical conditions can affect speaking, understanding, memory, problem-solving, reading, writing, or swallowing.
The practical focus becomes more immediate:
Paediatric focus | Adult focus |
|---|---|
Development and readiness | Recovery and adaptation |
Play, school, and peer participation | Home, work, safety, and independence |
Family concern about milestones | Functional concern after loss of skill |
Growth over time | Return to daily life or compensation |
A school-age child may be assessed for difficulty retelling a story or following classroom instructions. An adult may be assessed for whether they can manage a conversation with a pharmacist, remember a sequence at work, or safely eat and drink.
When learning problems and language overlap in school-aged children, it can help to understand related pathways such as assessments for learning disabilities, because referral questions often intersect.
Interpreting Results and Planning for Care
When assessment ends, families often expect a simple yes-or-no answer. Real interpretation is more careful than that.
The SLP has to pull together structured scores, observations, case history, and functional impact. Sometimes all the pieces point clearly in one direction. Sometimes they don't. A child might perform weakly on one formal task but communicate effectively in conversation. An adult might score within expected limits on brief items while still struggling in complex daily interactions.
What a report should actually tell you
A useful report usually answers these questions:
What was assessed
What the clinician observed
Which strengths stood out
Which difficulties affected daily communication
Whether the findings support a diagnosis or clinical profile
What to do next
If you're reading a report and can't tell what the person should work on tomorrow, the report probably needs clearer interpretation.
Turning findings into goals
Treatment planning works best when goals are practical and shared. Instead of writing a vague goal like “improve language,” the clinician should target something functional.
Examples:
A child will answer classroom “why” questions with support.
A student will produce specific speech sounds clearly in conversation.
An adult will use a memory strategy during phone calls.
A person with aphasia will retrieve key words needed for home routines.
Collaboration matters. The family may care most about dinner-table conversation. The teacher may care about narrative skills. The adult client may care about returning to work. The SLP has to align those priorities into a plan that is realistic and measurable.
Clinical reminder: Diagnosis matters, but treatment goals should still sound like real life.
For families looking ahead to therapy pathways, Orange Neurosciences has a helpful overview of speech therapy in Canada, including how assessment findings connect to intervention planning.
Good assessment doesn't end with “here are the results.” It ends with “here's what these results mean, and here's what we do next.”
Augmenting Assessments with Modern Technology
Traditional assessment is thorough, but it can also be time-intensive. Clinicians have to gather history, observe behaviour, administer tools, score results, and then decide whether the communication difficulty reflects a language disorder, a speech issue, a cognitive problem, or some combination.
That's where modern digital tools can help. They don't replace clinical judgement. They sharpen it.
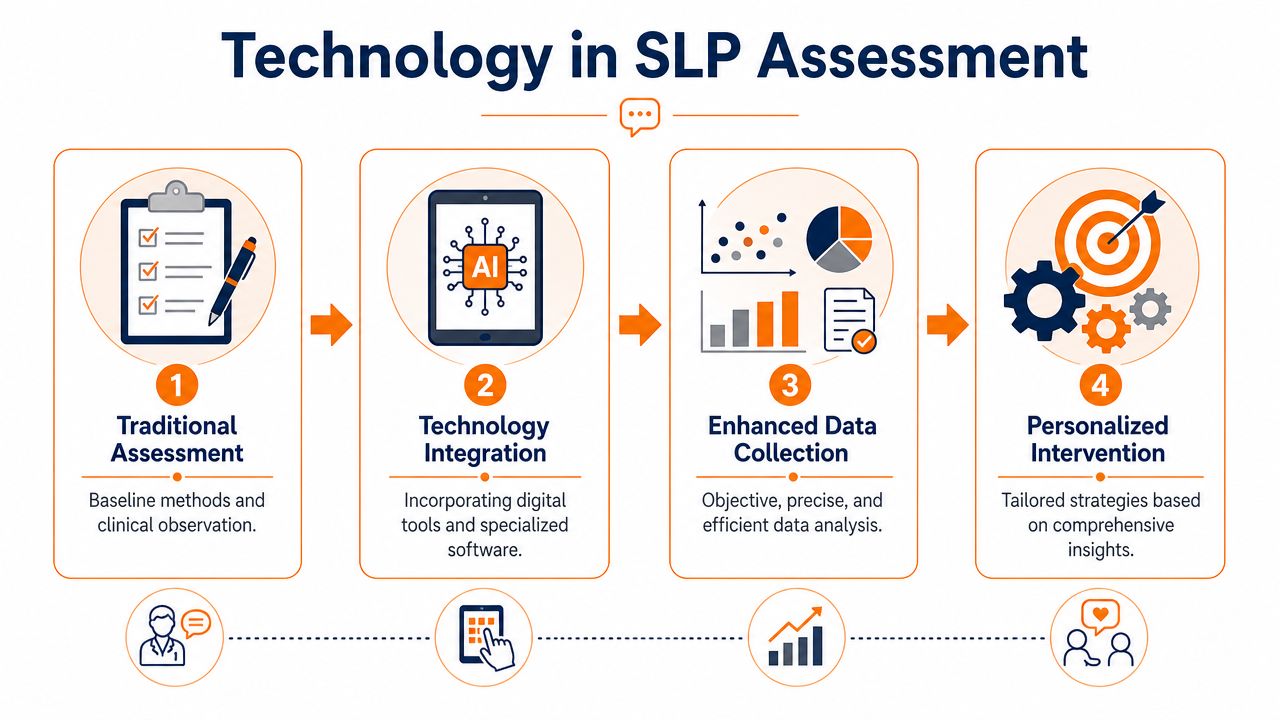
Where AI-supported tools fit
In speech and cognitive care, technology can support assessment by:
Flagging patterns earlier when attention, processing speed, or memory may be affecting communication
Providing objective baseline data that helps with triage and referral decisions
Supporting repeat measurement so clinicians can track change over time
Reducing guesswork when symptoms overlap across language, learning, and cognition
For example, a rapid cognitive screen may reveal that a person's language difficulty is partly driven by slowed processing or reduced working memory. That changes how the SLP interprets test behaviour and how therapy is planned.
One option in this space is Orange Neurosciences, which offers AI-powered cognitive assessment tools such as OrangeCheck to provide objective profiles across areas like attention, memory, executive function, processing speed, and eye-hand coordination. Used appropriately, tools like these can help clinicians decide whether more detailed evaluation is warranted and can add useful context to communication assessment. If you want to explore that category further, their guide to cognitive assessment tools is a practical starting point.
Technology is most useful when it answers a focused clinical question. It should make the workflow clearer, not more complicated.
If you're trying to make sense of communication concerns, or you want a faster, more objective way to support assessment decisions, visit Orange Neurosciences. Their resources and assessment tools can help families, educators, and clinicians build a clearer next step and move from uncertainty to informed care.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation