Patient Compliance vs Adherence: Boost Outcomes 2026

A patient nods through the visit, repeats the plan accurately, and leaves with every appearance of buy-in. Two weeks later, the refill is late, the home exercise sheet is untouched, and the follow-up reveals something more complicated than “didn't listen”. The instructions were clear. The plan still failed in real life.
That gap sits at the centre of patient compliance vs adherence. For clinicians, it's not a language preference. It changes how we assess barriers, how we structure follow-up, and how we judge outcomes. If the care model assumes obedience, we tend to label breakdowns as patient failure. If the care model assumes partnership, we start asking better questions about memory, motivation, cost, workflow friction, family support, and cognitive load.
In modern practice, especially in neurology, rehabilitation, developmental care, and chronic disease management, adherence is the more useful lens. It reflects how people manage treatment outside the clinic. It also opens the door to practical interventions that fit the patient rather than restating the prescription.
Beyond the Prescription Pad
A common scene in clinic goes like this. A patient with a chronic condition understands the medication schedule, agrees that therapy matters, and sincerely intends to follow through. Then work shifts change, sleep becomes erratic, the instructions compete with daily stress, and the plan starts slipping in small ways that aren't obvious until symptoms return.
That's why the old framing of “non-compliant patient” often misses the underlying clinical problem. In practice, patients may want to follow the plan and still struggle to execute it consistently. This is especially visible when treatment requires repeated action over time: medications, home programmes, cognitive exercises, follow-up appointments, dietary changes, or pacing strategies after brain injury.
A familiar example from daily practice
Consider a patient recovering from a neurological event who's given a simple-looking routine: take medication at set times, complete brief cognitive tasks, avoid overexertion, and return for reassessment. On paper, it's manageable. In reality, attention lapses, fatigue, poor working memory, or low confidence can disrupt every step.
Clinicians see this pattern across settings:
Medication plans get derailed by timing errors rather than refusal.
Home exercises fade when patients don't understand what progress should feel like.
Follow-ups are missed because scheduling itself becomes one more executive function task.
Caregiver-supported plans weaken when roles were never clearly negotiated.
A client-centred care approach becomes more than a values statement. It gives the clinician a practical starting point: stop asking only whether the patient followed instructions, and ask what made follow-through hard.
Patients often don't need a firmer lecture. They need a care plan that matches how they think, remember, organise, and live.
The point isn't to lower standards. It's to build plans that patients can carry out between visits. That's the shift from instruction to implementation, and it's where adherence becomes clinically useful.
The Critical Shift from Following Orders to Partnership
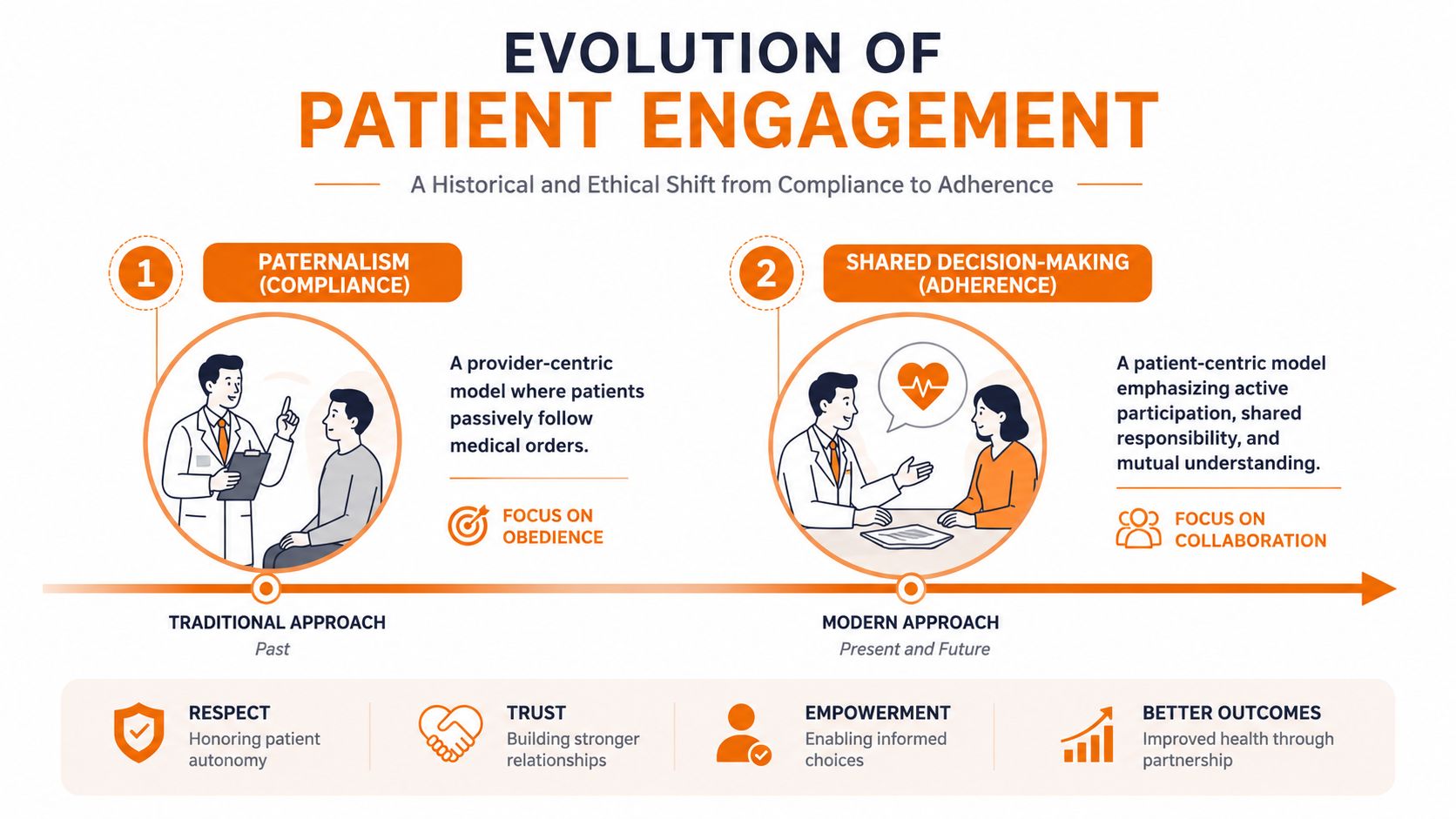
Early medical language treated the patient's role as straightforward: receive expert advice and follow it. That's the logic of compliance. It centres the provider's instructions and measures success by obedience. The model is simple, but it assumes that understanding automatically produces action.
A more modern model recognises that treatment works only when the patient can integrate it into daily life. Adherence was formally defined as behaviour matching “agreed recommendations” between provider and patient, rather than matching the prescriber's orders, as outlined in the European Patients' Forum discussion of adherence, compliance, and concordance. That distinction matters in the United States, where 75% of Americans struggle to follow medication instructions correctly, contributing to 125,000 deaths annually and costing the healthcare system up to $300 billion annually, according to that same source.
What changes when language changes
The terminology shift did more than tidy up medical vocabulary. It changed the ethical centre of care.
Under compliance, the implied questions are usually:
Did the patient obey instructions?
Did they take the medicine as told?
Did they attend as directed?
Under adherence, the questions become more clinically productive:
Was the plan mutually understood?
Did the patient have a meaningful choice?
What barriers blocked execution?
What support would make follow-through realistic?
This is one reason continuity matters so much. A fragmented handoff can turn a reasonable care plan into a series of disconnected tasks. In settings trying to improve this, a stronger continuity of care model gives patients fewer opportunities to fall between visits, teams, and instructions.
Partnership is operational, not sentimental
The best clinicians already know this. Shared decision-making isn't soft medicine. It's structured medicine. It means agreeing on a plan the patient can explain, accept, and carry out.
A useful analogy is the difference between issuing a route and planning a route. Compliance says, “Take this road.” Adherence says, “Given traffic, timing, and what you can manage, what route will you take and maintain?” Digital communication tools can support that kind of follow-through when they help clinicians personalise outreach, which is why some teams look at platforms such as Ekipa AI's healthcare professional engagement platform to coordinate timely, relevant contact with care stakeholders.
Clinical implication: Once you shift from compliance to adherence, missed follow-through stops being a verdict on the patient and becomes a signal to reassess the plan.
That shift leads directly to better measurement, better conversations, and better care design.
Compliance vs Adherence A Head-to-Head Comparison
The language overlap between the two terms causes problems in practice. Teams may use “compliance” and “adherence” interchangeably, then wonder why they aren't identifying the true cause of treatment failure. The distinction becomes clearer when you compare what each model assumes.
Dimension | Patient Compliance | Patient Adherence |
|---|---|---|
Patient role | Passive recipient of instructions | Active participant in care decisions |
Provider role | Director of treatment | Partner and guide |
Core assumption | Success depends on obedience | Success depends on agreement and fit |
Primary question | “Did the patient follow orders?” | “Could the patient sustain the agreed plan?” |
View of barriers | Secondary, sometimes overlooked | Central to assessment and follow-up |
Communication style | One-way explanation | Two-way discussion and negotiation |
Measurement focus | Immediate conformity | Ongoing implementation and persistence |
Response to failure | Risk of blame | Investigation and redesign |
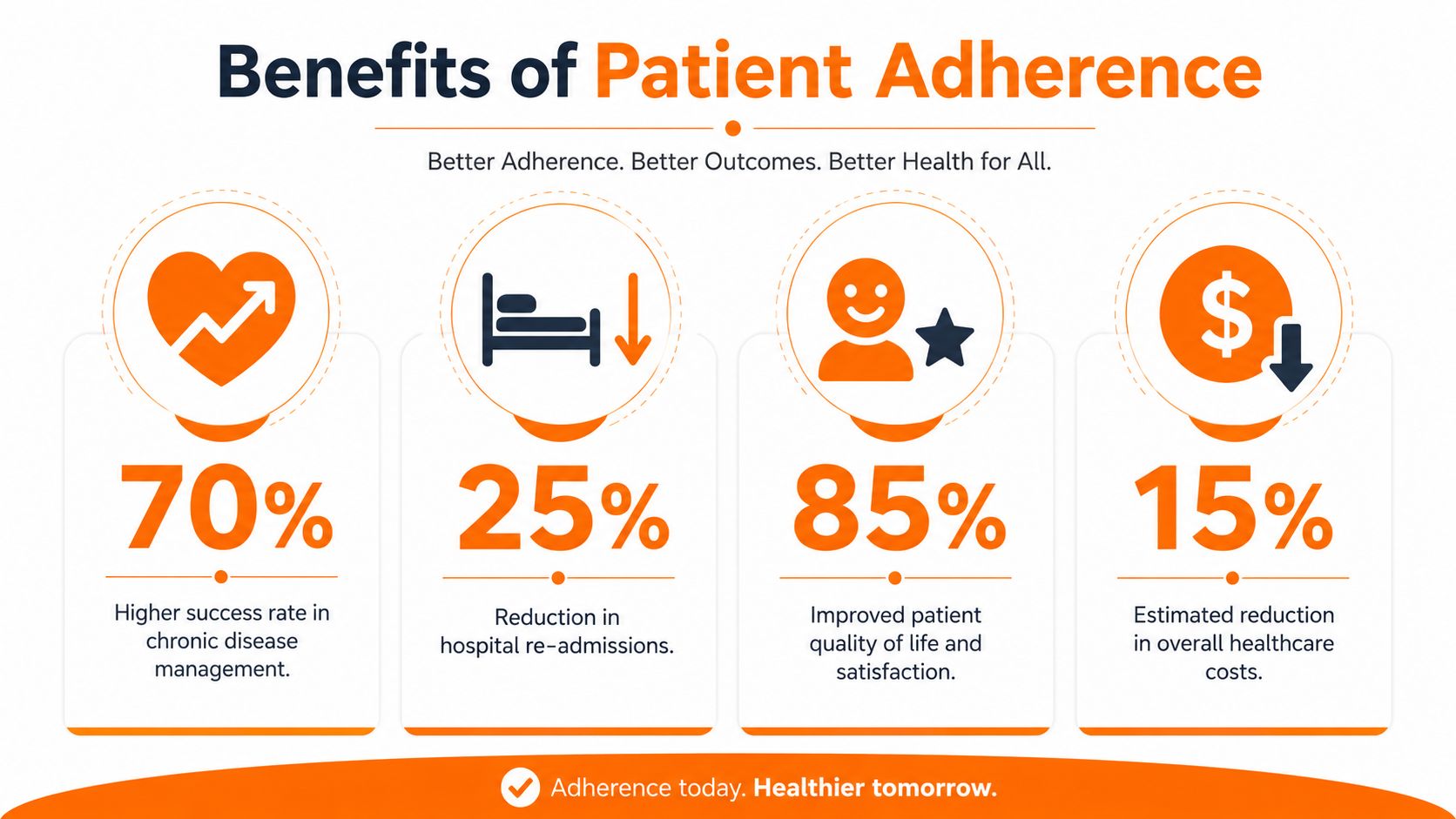
The clinical impact isn't theoretical. A meta-analysis found an overall outcome difference of 26% between high and low adherence, and in the United States 50% or fewer of patients continue with prescribed therapy after one year. The same analysis also notes that the typical benchmark for “adherent” behaviour is 80%, which is why this threshold matters in treatment evaluation and quality review, according to the PubMed summary on adherence and clinical outcomes.
Where compliance breaks down
Compliance works best when treatment is short, simple, and externally supervised. It struggles when care depends on repeated decisions made at home without immediate clinician oversight.
Take two examples:
Short antibiotic course: Compliance language may be enough if the task is finite and the instructions are simple.
Long-term neurorehabilitation plan: Compliance becomes too narrow because success depends on motivation, fatigue management, reminders, caregiver support, symptom tracking, and sustained participation.
In long-horizon care, the phrase “non-compliant” can shut down inquiry too early. It compresses many different realities into one label.
A patient who forgets doses, a patient who fears side effects, and a patient who cannot organise a multi-step routine are not facing the same clinical problem.
What adherence measures better
Adherence better reflects modern treatment demands because it includes execution over time. It also aligns with how clinicians already think in chronic care. We don't just ask whether a patient started treatment. We ask whether they maintained it, understood it, and adapted it appropriately.
A practical frame for patient compliance vs adherence is this:
Compliance measures instruction-following.
Adherence measures negotiated follow-through.
Persistence measures how long the patient remains on the plan.
That difference changes charting, counselling, and workflow design. It also changes what teams do after a lapse. In a compliance model, the intervention may be repetition. In an adherence model, the intervention is more often simplification, education, timing adjustment, caregiver involvement, or barrier removal.
A better question for case reviews
When a patient doesn't improve, many teams still ask, “Were they compliant?” A more useful question is, “What made adherence difficult, and did we identify it early enough?”
That question is more respectful. It's also better medicine.
Why Adherence Delivers Superior Clinical Outcomes
Adherence performs better because it treats behaviour as something clinicians can shape, not merely judge. When patients help build the plan, they're more likely to understand what matters, what trade-offs they're accepting, and what to do when routines are disrupted.
Trust changes execution
This is one of the strongest practical reasons to move beyond compliance language. California providers have emphasised that “trustful patient-provider relationships are at the centre of improving medication adherence”, and that seamless workflow integration with real-time decision support enables faster, better-informed care plans that strengthen that trust, as discussed in this California-focused review on medication adherence.
Trust affects ordinary clinical moments:
whether a patient admits they missed doses
whether they disclose side effects early
whether they ask for a simpler plan
whether they return before a small problem becomes a crisis
Without trust, patients often perform agreement in the room and abandon the plan at home.
Adherence builds self-efficacy
Patients are more likely to continue behaviours they can connect to visible benefit. This matters in rehabilitation and cognitive care, where progress may be gradual and where motivation can drop if the patient can't see the point of repeated work. That's why programmes that make progress legible tend to support better follow-through.
A useful rehabilitation principle is simple: make gains visible, make tasks proportionate, and make the next step obvious. That's part of why tools that support trend tracking and informed follow-up fit so well with a more structured rehabilitation and performance pathway.
If the care plan feels like a series of disconnected chores, adherence drops. If it feels like a coherent path with feedback, patients stay engaged longer.
Soft skills produce hard outcomes
Clinicians sometimes separate “communication” from “clinical care” as though the former is optional polish. It isn't. Shared decision-making, explanation quality, and timely follow-up are part of treatment delivery. They determine whether the patient can implement the plan outside supervised settings.
This is why adherence usually outperforms compliance in chronic and complex care. It connects motivation to understanding, and understanding to action. It also gives clinicians a framework for fixing what isn't working before the treatment itself gets blamed.
Practical Strategies to Cultivate Patient Adherence
Teams don't improve adherence with a single reminder system or one better handout. What works is a set of coordinated habits that reduce friction, reveal barriers early, and make progress easier to sustain.

Chronic disease management programmes have found that successful strategies include team-based care, cost reduction, and health information technology tools that automate monitoring and visualise trends to improve patient understanding of benefits, according to the CDC report on medication adherence strategies. Those principles transfer well to neurological and cognitive care.
Behavioural tactics that work in busy clinics
Behaviour change starts with conversation, but not all conversations are equally useful.
Use motivational interviewing for ambivalence: If a patient says they want to improve but keeps postponing therapy, don't repeat the instruction louder. Ask what makes the plan hard to maintain and what they would change first.
Set one visible target at a time: A patient leaving rehab with six new expectations is likely to fail on several. A patient leaving with one primary daily task and one backup plan usually does better.
Normalise difficulty: Patients are more honest when missed steps aren't treated as disobedience. That honesty gives you workable data.
A practical example: instead of “Do your exercises every day,” try “Which time of day is most realistic, and what usually gets in the way?”
Educational methods that reduce confusion
Many breakdowns in adherence are really breakdowns in interpretation.
A few changes help immediately:
Use teach-back: Ask the patient to describe the plan in their own words.
Cut information into steps: One page with priorities is often more useful than a dense discharge packet.
Explain the benefit in plain terms: Patients stick with routines better when they know what the routine is supposed to improve.
For patients or caregivers looking for a consumer-friendly supplement to in-clinic education, these PepFlow tips for medication consistency are a reasonable example of how reminder and routine ideas can be translated into everyday use.
Workflow and environmental supports
Many practices either gain traction or lose it at this point.
Simplify the regimen when possible: Fewer moving parts usually beats a theoretically optimal but unwieldy plan.
Build team follow-up: Nurses, therapists, pharmacists, educators, and caregivers often see barriers before the prescriber does.
Show trends, not just instructions: Patients engage better when they can connect effort with observable change.
Practice pattern: When teams automate routine monitoring and reserve clinician time for problem-solving, adherence conversations become more specific and less reactive.
The important trade-off is this: every added layer of monitoring creates data, but too much complexity can burden staff and patients. The best systems don't just collect information. They turn it into simpler decisions.
Supporting Adherence with Digital Cognitive Assessment
Some patients don't fail a treatment plan because they disagree with it. They fail because the plan asks for cognitive skills they currently can't reliably use. That's where many adherence efforts stall. The reminders are sent, the education is given, the follow-up is scheduled, and the underlying problem still goes unrecognised.

Cognitive barriers are often operational barriers
A patient with reduced working memory may understand instructions in clinic and forget the sequence by evening. A patient with executive dysfunction may know exactly what to do and still be unable to organise the steps. A patient with attention problems may start the routine and repeatedly lose the thread.
Those are not minor details. They determine whether adherence strategies should focus on reminders, simplification, caregiver scaffolding, environmental cueing, or redesign of the treatment schedule itself.
Examples from practice make this clear:
Memory weakness: Use visual pill organisers, written sequencing, and same-time routines instead of relying on verbal recall.
Executive function difficulty: Reduce multi-step tasks and assign one initiation cue.
Attention variability: Keep instructions short, concrete, and tied to predictable anchors in the day.
Processing speed issues: Allow more time for explanation and avoid stacking too many decisions into one visit.
Why digital tools matter here
Multimodal patient programmes that combine technology with personalised education and structured follow-ups showed an odds ratio of 2.48 for improved adherence compared with standard care, according to the systematic review on interventions to improve adherence. The practical lesson is not that technology replaces clinical judgement. It's that technology can make adherence barriers visible earlier and support more appropriate follow-through.
For clinicians working with neurocognitive complexity, digital cognitive assessment proves especially useful. A platform such as Orange Neurosciences can generate objective cognitive profiles in under 30 minutes across domains such as attention, memory, executive function, perception, processing speed, and eye-hand coordination, then feed that information into more personalised intervention planning. In that setting, a digital cognitive assessment workflow isn't just about measurement. It helps match the adherence strategy to the patient's actual cognitive capacity.
The question is no longer “Why didn't this patient follow the plan?” It becomes “Did the plan depend on cognitive strengths the patient doesn't currently have?”
The practical payoff
When cognitive barriers are identified early, clinicians can adapt the plan before repeated non-adherence erodes trust. That often means fewer assumptions, clearer delegation to caregivers, better timing, and more realistic self-management tasks.
This is the unique advantage of bringing cognitive assessment into the adherence conversation. It turns vague frustration into specific, treatable obstacles.
Building an Adherence-Focused Practice in 2026
An adherence-focused practice doesn't ask patients to be more obedient. It asks clinicians to build plans that fit the realities of cognition, motivation, daily routine, and long-term follow-through. That's a higher standard, but it's also a more workable one.
The shift matters most in complex care. Neurology, rehabilitation, developmental practice, senior care, and chronic disease management all depend on actions that happen far from the clinic. If those actions are hard to remember, organise, or sustain, better wording on the discharge sheet won't solve the problem. Better design might.
A mature adherence model usually includes three things: collaborative planning, early identification of barriers, and systems that make progress visible. That same logic applies beyond medication management. For example, in musculoskeletal rehabilitation, structured educational resources such as this Complete guide to scoliosis management can help patients understand why consistency matters across a longer treatment arc.
Operationally, the next step for many teams is straightforward. Review where your patients tend to fall off, decide which barriers are behavioural versus cognitive, and make it easier to track both day-to-day engagement and longer-term continuation. If your service model needs a cleaner intake and follow-through pathway, a more organised registration and enrolment workflow can support that shift from the first contact onward.
If you want to identify hidden cognitive barriers behind missed follow-through, explore how Orange Neurosciences supports rapid cognitive assessment, targeted therapy planning, and ongoing progress tracking. You can also reach out by email through the website to discuss how an adherence-focused workflow could fit your clinical setting.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation