Elevate Rehabilitation and Performance: Boost Outcomes
Apr 12, 2026
Many rehabilitation teams are in the same spot. A patient says their thinking feels “better”, but they still can’t manage work demands, follow a busy home routine, or keep pace in therapy. Another says they’re only “a bit foggy”, yet their return to driving or sport keeps slipping.
That gap between what a patient reports and what they can do creates friction everywhere. It slows planning, muddies handoffs between clinicians, and makes progress reviews feel argumentative instead of clear. In a busy centre, that ambiguity is expensive in time and hard on trust.
In advanced rehabilitation and performance settings, that's where digital cognitive assessment starts to matter. Not as a replacement for clinical judgement, and not as a shortcut diagnosis, but as a way to pin down what’s happening well enough to treat it properly.
From Subjective Guesses to Objective Certainty
A post-concussion athlete tells you concentration is “mostly fine”. A stroke survivor says memory is “not too bad now”. Their family isn’t convinced. Your treatment notes show effort, but function hasn’t moved in the way everyone expected.
That’s a familiar clinical problem. Subjective reports are useful, but they’re incomplete. Patients often under-report, over-estimate, or describe symptoms in language that doesn’t map neatly to treatment decisions.
Where the uncertainty shows up
In practice, the trouble isn’t just that symptoms are vague. It’s that vague symptoms lead to vague plans.
A patient who says they feel mentally slow might have difficulty with processing speed, sustained attention, visual scanning, working memory, or fatigue regulation. Those are not the same issue, and they shouldn’t get the same intervention.
When clinicians rely only on conversation and broad observation, several things tend to happen:
Goals stay too general. “Improve focus” sounds reasonable, but it doesn’t tell the team what to train.
Progress reviews become subjective. One therapist sees improvement. Another sees inconsistency.
Discharge decisions get harder. The patient feels better, yet work, school, or sport still exposes deficits.
Practical rule: If you can’t describe the deficit precisely, you’ll struggle to prescribe the right task load, frequency, and progression.
This isn’t just a cognitive rehab issue. Across rehabilitation, stronger care tends to follow better measurement. The same broader logic appears in the scientific evidence supporting advanced rehabilitation methods, where objective inputs help clinicians move beyond assumption and towards targeted intervention.
What objective assessment changes
A structured cognitive baseline gives the team a common language. It tells you whether the main limiter is attention control, memory load, executive efficiency, visual perception, or response speed. That changes the next appointment immediately.
It also helps with expectation management. Instead of telling a patient “let’s keep working on brain recovery”, you can explain what is holding them back and why the treatment plan looks the way it does.
For teams that are still deciding where to begin, a plain-language overview of https://www.orangeneurosciences.ca/guide/what-is-cognitive-assessment is a useful starting point for framing cognitive assessment within routine care.
Building Your Foundation on Cognitive Baselining
Modern rehabilitation works better when baselines are clear. That applies to range, force, gait, pain behaviour, and it applies just as much to cognition. If a clinic wants to enhance rehabilitation and performance rather than just deliver sessions, it needs a defined starting point.

The strongest argument for baselining is operational, not philosophical. Once a clinic can measure something consistently, it can organise staffing, track progress, and adjust care with less delay.
Data changes decisions
That pattern is already visible in rehabilitation businesses that made the shift to live data. A Sports Performance clinic in Nevada moved from manual spreadsheets to real-time analytics, and one-on-one training sessions now account for 40% of total revenue, with the team using data to monitor capacity, track rebooking rates, and make strategic decisions that support growth and patient outcomes (Mindbody customer story on a Sports Performance clinic's data-driven analytics use).
The lesson for cognitive care is straightforward. When data is available at the point of decision, the team doesn’t have to wait for vague trends to become obvious. It can respond earlier.
For cognitive rehab, a baseline should answer a few practical questions:
What is weak right now? Attention, memory, executive control, processing speed, perception, eye-hand coordination, or a mix.
What is preserved? Preserved strengths matter because they help you choose compensatory strategies.
What should change first? Not every deficit needs equal priority in the first block of care.
What a useful baseline looks like
A useful baseline is brief enough to fit workflow, broad enough to catch the main domains, and stable enough to support repeat testing. If it takes too long, staff will bypass it. If it’s too shallow, the report won’t guide treatment.
That’s why reliability matters. If you’re building care around repeated measures, test consistency matters as much as test convenience. A practical review of this issue is available at https://www.orangeneurosciences.ca/guide/reliability-test-retest.
A good baseline also needs context. Raw scores by themselves don’t make a plan. Clinicians still need to interpret findings against referral reason, fatigue, language load, pain, medication effects, and the patient’s actual functional complaints.
A baseline isn’t there to impress anyone. It’s there to reduce guessing at the exact point where treatment choices are made.
Baselining improves communication
Baselines also clean up team communication. The physio, occupational therapist, physician, kinesiologist, and family can align around the same profile instead of carrying separate impressions.
That tends to improve three things in day-to-day practice:
Tighter goal setting “Improve memory” becomes “improve delayed recall for multi-step home exercise instructions”.
Better pacing A patient with reduced processing speed may need fewer instructions per set and more structured transitions.
Clearer progress reviews Reassessment has a benchmark. You’re not comparing today’s session to a memory of last month.
Integrating Assessment Into Your Workflow
A patient finishes the first evaluation with clear physical goals, but the home program still falls apart by week two. The issue is not motivation. The patient forgot the sequence, fatigued halfway through the instructions, and could not keep up once the session became more complex. If cognitive assessment sits outside the initial workflow, the team often discovers that problem late, after missed progress, extra visits, and a preventable rewrite of the plan.
The operational fix is simple. Put cognitive assessment inside the patient flow you already use, with a clear handoff from screening to interpretation to treatment decisions.
Start at intake, not after the second visit
Intake is the best point to decide whether cognitive screening belongs in the first evaluation block. Referral reason usually gives enough direction. Concussion, stroke, TBI, neurological illness, persistent pain, post-operative recovery, and long periods of deconditioning can all affect attention, memory, processing speed, and follow-through.
Screen when the patient reports problems such as:
Reduced concentration during work, school, or reading
Memory lapses with appointments, medication, or home exercise steps
Slower decision-making in busy or dual-task situations
Mental fatigue that shortens sessions or limits carryover
That timing matters because it changes what happens next. The goal is not to collect another report. The goal is to shape instructions, pacing, cueing, and progression before the first treatment block starts.
Assign ownership clearly
Implementation slips when responsibility is spread across the whole team. In practice, one person needs to own the process.
That role is often a rehab assistant, occupational therapist, or intake clinician. Their job should be specific:
confirm the patient is appropriate for testing
place the patient in the right environment
make sure results enter the chart or case review process
alert the treating clinician when the profile is ready
This is also where clinics either gain consistency or lose it. A named owner reduces missed assessments, uneven administration, and delayed review.
Make the environment consistent
Digital assessment does not require a lab, but it does require control over the testing conditions.
A quiet office, a private corner, or a dedicated tablet station is usually enough. What matters is protecting the task from interruption. A timed attention measure completed beside a ringing front desk is partly measuring distraction tolerance, not just cognition.
A few ground rules usually solve the problem:
Use the same device type when possible
Protect the testing block from routine interruptions
Explain the purpose clearly so the patient understands that the assessment supports treatment planning
Keep administration routine. Staff are more likely to complete it correctly when the setup feels ordinary and repeatable.
Put results where clinicians already work
Assessment adds friction when the report sits in a separate dashboard that nobody checks during care planning. Results need a defined place in the chart, and the treatment note should show how those findings changed the plan.
The workflow standard is straightforward. Review the cognitive profile during the same decision point where goals, dosing, home exercise structure, and education strategy are set. That is the practical side of client-centered care in rehabilitation planning. Data should change what the patient receives, not just what the clinic stores.
Operational integration also affects admin time. In a StrataPT case study on documentation and billing efficiency in a Physical Therapy clinic, optimized EMR use was associated with 80% faster patient documentation time and a 50% reduction in billing and administration time. The same case study reports that automating intake and charting cut manual entry from 20 to 30 minutes to under 5 minutes per session. Those numbers come from documentation systems, not cognitive testing specifically, but the lesson is relevant. If assessment outputs feed directly into charting, review happens faster and adoption tends to hold.
A clinic workflow that works in practice
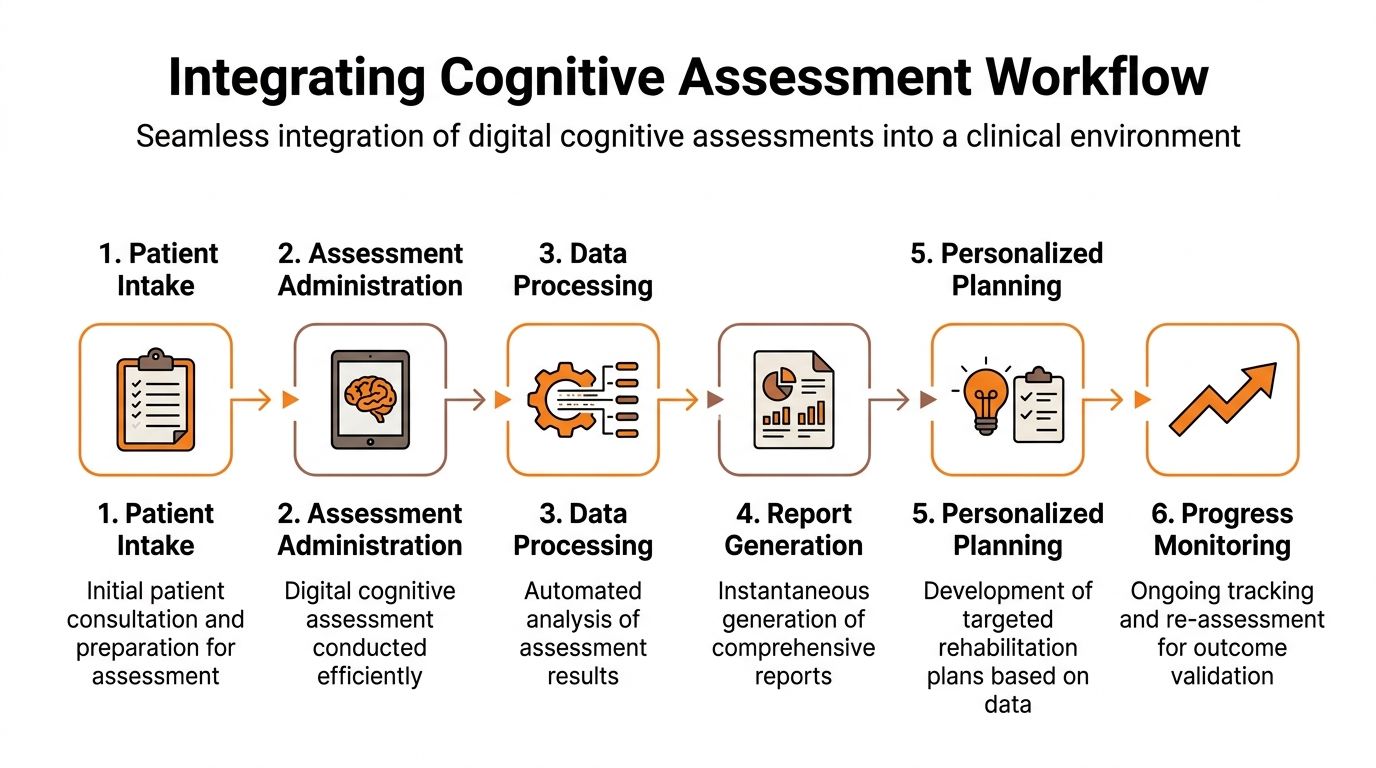
Many teams do well with a simple six-step model:
Stage | Who handles it | What happens |
|---|---|---|
Referral review | Intake coordinator | Flags likely cognitive concerns |
Initial booking | Admin team | Adds assessment block to first evaluation window |
Assessment administration | Assigned staff member | Runs test in a quiet, standardised setting |
Result review | Treating clinician | Interprets findings against functional demands |
Care plan update | Clinical lead or therapist | Changes cueing, pacing, instruction style, and targets |
Reassessment booking | Front desk or therapist | Sets the review date before the patient leaves |
The step many articles skip is the care plan update. That is where the platform earns its place. If a clinic uses a system such as Orange Neurosciences, assessment, reporting, and targeted training can sit in one care pathway instead of being split across separate tools. That makes it easier to connect a finding to an intervention while the case is still active.
Avoid the operational mistakes that slow adoption
The common failures are rarely technical.
Late introduction Assessment gets ordered only after progress stalls, so the report arrives after the treatment pattern is already set.
Over-testing Staff repeat measures too often and create noise instead of a useful comparison point.
Weak handoff The report is completed, but no one changes teaching strategy, exercise structure, or between-session support.
The last problem causes the most waste. Assessment only improves care when the clinic has a defined path from score to action.
Translating Cognitive Data Into Actionable Care Plans
Collecting cognitive data is the easy part. The hard part is turning that report into treatment choices that change function.
Rehabilitation teams already know this principle from physical care. In low back pain management, early PT guided by initial assessment reduces one-year surgery risk by 40 to 60% and lowers costs by 30% compared with delayed care, because the process starts with classification and then moves into individualized exercise rather than generic advice (A PT Fit clinic on early physical therapy for low back pain).
Cognitive care needs the same discipline. Assess first. Classify the problem. Match intervention to the finding.
The report should answer what to do next
When clinicians review a cognitive profile, they should ask four treatment questions:
What domain is most likely limiting daily function?
Which deficit is primary, and which problems are secondary?
What task demands should be reduced, increased, or modified?
How will the patient notice improvement in real life?
A patient with weak working memory may look inattentive during teaching. A patient with slow processing speed may appear forgetful because instructions outrun them. A patient with executive difficulty may know the exercises but fail to sequence them independently.
Those distinctions matter because they change the intervention.
Mapping Cognitive Domains to Targeted Interventions
Cognitive Domain | Example Assessment Finding | Targeted Intervention Strategy | Functional Goal |
|---|---|---|---|
Attention | Difficulty sustaining focus across repeated task demands | Use short, structured tasks with controlled distractions, then progress to longer task blocks | Follow a treatment session without frequent redirection |
Working memory | Trouble holding and manipulating multi-step information | Practise graded recall and sequencing tasks, then apply to home programme instruction | Complete a multi-step home routine accurately |
Processing speed | Slowed responses despite accurate understanding | Reduce information load per instruction, use timed visual or motor-cognitive drills, then increase pace gradually | Respond efficiently in conversation, work tasks, or sport drills |
Executive function | Poor planning, set-shifting, or error correction | Use tasks requiring strategy, rule changes, and self-monitoring with therapist feedback | Organise daily tasks and adjust when routines change |
Visual perception | Missed details, inefficient scanning, or spatial errors | Train visual search, scanning pathways, and environmental orientation tasks | Move through busy spaces and read information more reliably |
Eye-hand coordination | Inconsistent timing or targeting on visually guided actions | Use graded visuomotor tasks with speed and accuracy targets | Improve safe functional interaction with tools, devices, or sport equipment |
Use if-then planning
Care plans get sharper when the team writes them in if-then language.
If processing speed is the main limiter, then reduce verbal overload, use shorter instructions, and build speed through graded visual and decision tasks.
If working memory is weak, then stop relying on long verbal teaching and add written prompts, repetition, and chunked sequencing.
If executive function is impaired, then include planning tasks, error-detection demands, and routine-building rather than just drill repetition.
That keeps treatment linked to findings instead of habit.
For clinicians who want a stronger framework for this kind of treatment design, https://www.orangeneurosciences.ca/guide/client-centered-care is a useful reference because it keeps the plan tied to the person’s actual life demands rather than isolated test performance.
The report matters only when it changes the next exercise, the next cue, or the next home assignment.
A practical example from clinic flow
Consider a patient recovering from concussion who reports trouble returning to office work. Assessment shows relatively intact accuracy but reduced processing speed and fatigue under sustained attention demands.
A weak plan would say, “continue cognitive exercises”.
A strong plan would do the following:
Modify session delivery so instructions are brief and grouped.
Train the limiting domain with paced attention and response tasks.
Transfer into function by simulating email sorting, schedule review, or divided-attention office demands.
Grade return-to-work exposure around duration and complexity, not confidence alone.
That’s what assessment-to-intervention mapping looks like in practice.
Implementing and Monitoring Targeted Training Protocols
Once the plan is written, execution has to stay tight. Many programs drift at this point. The exercises exist, the patient is motivated, but the dosage, progression, and review process aren’t structured enough to create steady gains.
Good targeted training looks less like “brain games” and more like any other rehab protocol. It has a starting level, a progression rule, a stop rule, and a reassessment point.

Dose the task, not just the appointment
The first job is to set the right challenge level. If tasks are too easy, the patient gets false reassurance. If they’re too hard, performance collapses and adherence drops.
A practical protocol usually defines:
Session purpose Which domain is being trained today, and why that domain matters functionally.
Difficulty anchor What starting level the patient can complete with effort but without repeated breakdown.
Progression trigger What improvement tells you the task can become faster, more complex, or less supported.
Fatigue threshold When quality drops enough that continuing no longer trains the intended skill.
Digital platforms are useful here. They can adapt challenge more precisely than paper tasks, and they generate performance data without forcing the therapist to score everything manually.
Use real-time analytics to adjust early
Physical rehabilitation already shows the value of objective progress tracking. Advanced centres use tools such as ForceDecks to measure strength and asymmetry with instant reports, helping clinicians detect weaknesses early and turn data into practical strategy rather than waiting for problems to become obvious (Integrated Clinical S&C on jump analysis and objective rehab tracking (improve patient outcomes)...)).
The cognitive equivalent is to watch for patterns such as:
improving accuracy with unchanged speed
improving speed with falling accuracy
strong performance in quiet conditions but collapse under dual tasking
steady early gains followed by fatigue-driven inconsistency
Those patterns tell you whether to push pace, simplify demands, add context, or reduce session burden.
Keep training tied to function
Patients stay engaged when they can see why the task matters.
A person training divided attention after neurological injury should understand how that connects to cooking safely, managing a conversation in a busy room, or moving through a gym while processing instructions. A teenager after concussion should know why visual processing work matters for schoolwork and sport re-entry.
That link should appear in every plan note.
Don’t ask patients to trust abstract improvement. Show them the functional reason behind each training block.
A weekly review format that works
Use a short weekly review rather than waiting for a major reassessment.
Check performance trends
Look for consistency before intensity. If the patient improves only on their best day, the skill probably isn’t stable enough to progress.
Review symptom load
A patient may complete the task but pay for it later with headaches, irritability, or mental exhaustion. If symptom burden rises, the protocol may be over-dosed even when scores look acceptable.
Change one variable at a time
Progress either duration, complexity, distraction level, or pace. Don’t increase all of them together or you won’t know what helped and what hurt.
Example of closed-loop protocol management
A patient starts with short visual attention tasks and simple working memory drills. In week one, accuracy is good, but speed drops sharply as task length increases.
The clinician responds by keeping complexity stable and increasing duration only slightly. In the next block, the patient tolerates longer work without the same decline. Then the therapist introduces more real-world interference, such as conversation or background noise.
That’s closed-loop care. Assess, train, observe, adjust, repeat.
For teams building this style of structured progression, https://www.orangeneurosciences.ca/guide/cognitive-remediation-therapy gives a useful overview of how cognitive remediation can be applied in a treatment setting.
Measuring What Matters and Demonstrating Clear Outcomes
If a clinic invests time in digital cognitive assessment and targeted training, it has to prove value in language that different stakeholders understand. Patients want to know whether life is easier. Families want to know whether independence is improving. Referrers want evidence that the plan is specific. Clinic leaders want to know whether services are organised and defensible.
That means measuring outcomes on two tracks. Clinical outcomes and operational outcomes.
Measure clinical change in a way patients recognise
A score change matters only if it maps to function. The report should connect objective findings to tasks the patient cares about.
Useful outcome questions include:
Can the patient manage a busier environment without cognitive overload?
Can they follow multi-step instructions more independently?
Can they return to work, study, sport, or self-management with less support?
When clinicians write progress notes this way, reassessment becomes easier to explain. You’re not just saying a domain improved. You’re showing how that improvement changed behaviour.
Use data to support value conversations
Clear reporting also helps the business side of advanced rehabilitation and performance. It gives clinics a stronger basis for care recommendations, family updates, and referral communication.
The broader rehab field is already moving this direction. A useful example from physical care is how smart tech is changing physical therapy, where better measurement tools support better decision-making instead of relying only on feel.
That same principle applies in cognitive care. If a clinician can show baseline findings, targeted intervention, and reassessment-linked progress, the plan becomes easier to justify.
Build an outcome dashboard around a few essentials
Don’t drown the team in metrics. Use a short list that answers practical questions.
Outcome area | What to track | Why it matters |
|---|---|---|
Baseline impairment | Main affected domains | Clarifies treatment priorities |
Functional targets | Work, school, home, or sport goals | Keeps care patient-specific |
Training adherence | Completion and consistency | Shows whether poor progress is a dosing issue |
Reassessment trend | Direction of change over time | Supports progression or referral decisions |
Care plan changes | What was modified and why | Makes treatment reasoning visible |
Good reporting doesn’t mean reporting everything. It means reporting the few things that make decisions easier.
When results are unclear
Not every patient shows a clean upward line. That’s normal.
Sometimes cognitive scores stay flat while fatigue improves. Sometimes performance gets better in clinic before function improves at home. Sometimes results suggest the patient needs formal neuropsychological evaluation rather than more routine rehab training.
That isn’t failure. It’s exactly why measurement matters.
Common Questions About Adopting Digital Cognitive Tools
Clinicians usually don’t resist digital cognitive tools because they dislike data. They resist them because they’re trying to protect clinical standards, staff time, and patient trust. Those are valid concerns.
Is this a diagnostic tool
No. A digital cognitive assessment platform should be treated as a structured measurement and decision-support tool, not a standalone diagnosis.
That distinction matters. Screening and profiling can show patterns, identify areas of concern, and help determine whether further evaluation is warranted. Formal diagnosis still sits within the scope of the appropriate regulated professionals and fuller clinical process.
In practice, that means the platform informs treatment planning and referral decisions. It doesn’t replace neuropsychological evaluation when the case requires it.
How much staff training is needed
Usually less than teams fear, but more than vendors sometimes imply.
Staff don’t need advanced psychometrics to administer a well-designed digital assessment. They do need a clear protocol for set-up, patient instruction, troubleshooting, and result handoff. The main training issue isn’t test delivery. It’s interpretation discipline.
A sensible training roll-out includes:
Administration standards so testing conditions stay consistent
Interpretation boundaries so staff don’t overstate what the results mean
Workflow responsibilities so no assessment gets stranded outside the plan of care
If the platform is intuitive, most adoption problems come from inconsistent clinic process rather than staff inability.
What does return on investment usually look like
ROI should be judged in time, clarity, and treatment precision first.
A clinic benefits when the tool helps staff identify the primary limiter sooner, document more cleanly, and reduce avoidable delay in care planning. It also helps when progress reviews become easier to explain to patients and referrers.
The wrong way to think about ROI is “Will this software magically fix outcomes?” It won’t. It gives the team better information. The clinic still needs sound clinical reasoning and organised delivery.
How do you keep data privacy and compliance in view
Privacy shouldn’t be an afterthought added during procurement. It should be part of vendor review from day one.
Ask direct questions about data storage, user permissions, audit trails, consent processes, and how the platform supports compliance with the privacy obligations relevant to your setting, including PHIPA in Canada when applicable.
Operationally, clinics should also decide:
who can administer assessments
who can view reports
where results are stored in the record
how reassessment data is retained and shared
Does this work only in neuro settings
No. It’s most obvious in concussion, stroke, and brain injury, but cognitive load affects many rehabilitation pathways.
Patients with chronic pain, post-operative deconditioning, vestibular complaints, complex return-to-work cases, and older adults with declining confidence may all benefit from clearer cognitive profiling when function and self-management are under strain.
A practical overview of remote and digital use cases is available at https://www.orangeneurosciences.ca/guide/cognitive-assessment-online.
What assumption needs to change first
The biggest one is this: if a patient can describe their symptoms well, the team already understands the problem.
That assumption fails often. Patients describe experience. Clinicians need performance data. Both matter, but they aren’t interchangeable.
When a centre combines clear baselining, workflow discipline, intervention mapping, and repeated review, digital cognitive assessment stops feeling like an add-on. It becomes part of how the clinic delivers modern, defensible rehabilitation.
If you want to build a more measurable cognitive care pathway into your clinic, visit Orange Neurosciences to review the platform, explore how assessment and training fit into practice, or contact the team by email to discuss implementation in your setting.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation