Exercise for Concussion: Safe Recovery Guide 2026

The most common bad advice after a concussion is still “rest until all symptoms are gone.” That sounds safe. It often isn't helpful.
Modern concussion rehab has moved away from prolonged cocooning in a dark room and toward early, controlled, symptom-limited movement. The shift matters because patients don't just need protection. They need the right dose of activity, at the right time, with the right guardrails.
That's where exercise for concussion gets misunderstood. The problem usually isn't that people move too soon. It's that they either do far too much, or nothing at all, or they follow a generic handout that ignores dizziness, visual strain, neck pain, school demands, work demands, and how their symptoms behave.
Why Active Recovery Is the New Standard for Concussion

The old model was simple. Rest completely. Avoid activity. Wait.
The current model is more useful because it matches what clinicians now see in practice and what better evidence supports. In a study of over 3,000 children and adolescents with acute concussion, any physical activity within 7 days of injury was associated with a lower rate of persistent post-concussive symptoms at 28 days: 24.6% versus 43.5% in those who did no physical activity (study details).
That doesn't mean “go back to normal sport immediately.” It means complete inactivity is no longer the default prescription.
What active recovery actually means
Active recovery means introducing movement that stays below the person's symptom threshold. In practical terms, that usually starts with basic aerobic activity such as walking or a stationary bike, not sprints, not circuits, and not strength sessions.
A few examples:
Teen athlete with headache and light sensitivity: a short, easy walk indoors may be appropriate before any field work.
Office worker with mental fog and neck tension: a brief walk plus gentle mobility may be more realistic than a treadmill session.
Older adult with dizziness: seated or supported options are often safer than outdoor walking at first.
Recovery improves when patients stop treating all symptoms as a signal to stay still and start treating symptoms as data that guide dose.
Why the older “dark room” advice falls short
After the first short period of relative rest, over-resting can create its own problems. Patients often become more deconditioned, more anxious about movement, and less confident about returning to school, work, driving, exercise, or sport.
The better question isn't “Should this person rest or exercise?” It's “What kind of movement can they tolerate without provoking a meaningful setback?”
That shift changes clinical decision-making. It also changes patient education. When families understand that movement is part of rehab, they stop seeing every symptom bump as damage. They start seeing pacing as a skill.
For people trying to understand the legal and medical distinction between concussion and more severe traumatic brain injury after an accident, Mattiacci Law on TBI cases offers a useful plain-language overview. For a broader rehab framework, Orange's complete concussion management guide is a practical companion to clinical care.
The First 48 Hours and When to Begin Moving
The first two days matter. They just don't call for complete shutdown.
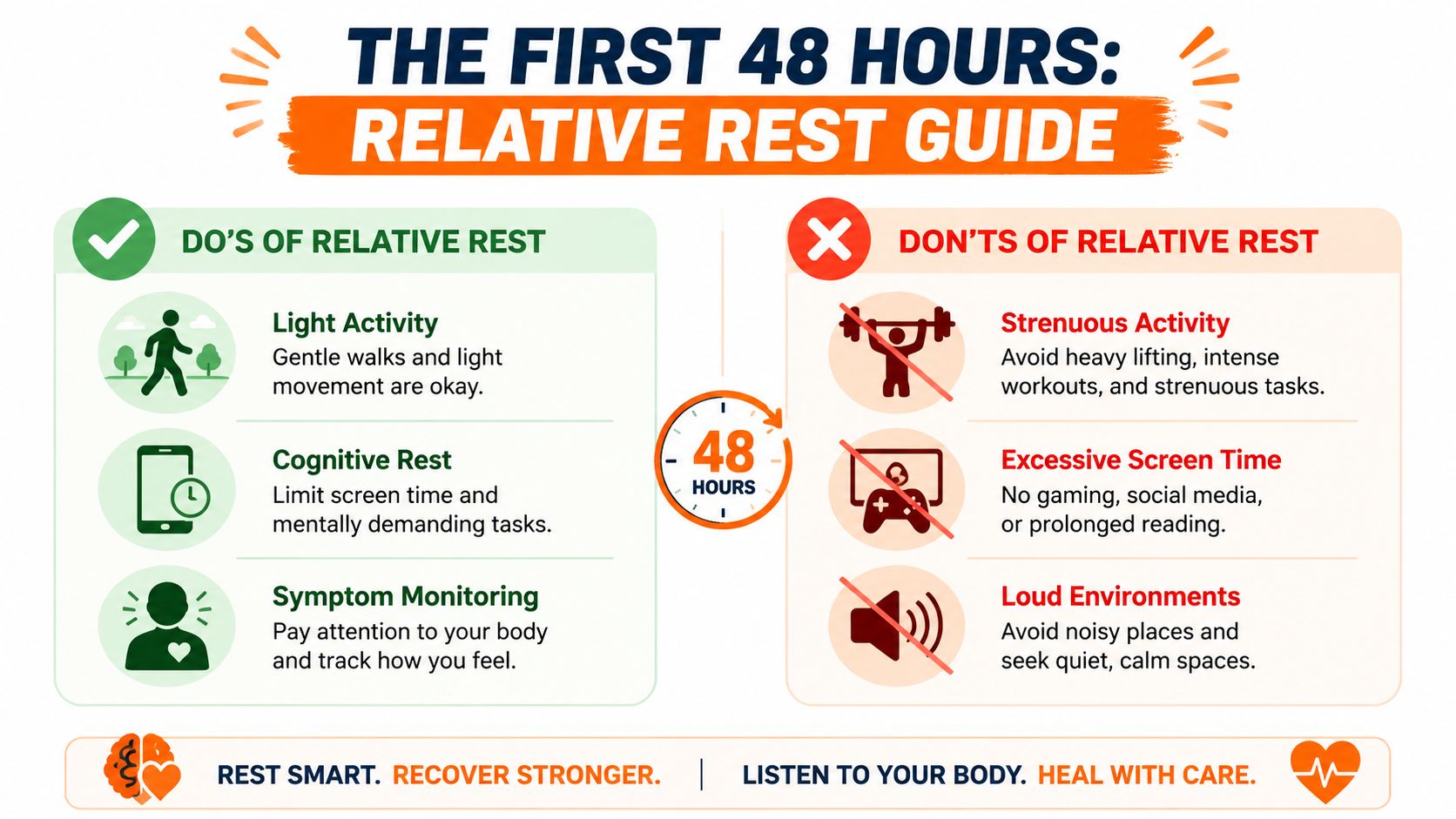
Current guidance supports 24 to 48 hours of relative rest, then a gradual start to light aerobic activity if symptoms remain manageable. Relative rest means reducing things that clearly aggravate symptoms while still allowing basic daily movement and quiet routine.
What relative rest looks like in real life
Think of relative rest as “calm, not coma.”
That usually includes:
Short, easy movement: brief walks around the home, gentle movement between rooms, simple daily tasks.
Reduced cognitive strain: less scrolling, less gaming, less prolonged reading, and less multitasking if those spike symptoms.
Quieter settings: lower noise, lower visual clutter, less rushing.
Basic self-monitoring: notice whether symptoms settle quickly or continue climbing.
What it does not include is lying in bed all day unless the person is medically unwell for another reason.
What to avoid early
A lot of early mistakes come from doing the wrong kind of effort, not just too much effort.
Avoid:
Heavy lifting: early resistance work increases strain and isn't the right starting point.
Hard cardio: intervals, hill running, fitness classes, and “sweating it out” approaches.
Long screen sessions: especially if they trigger headache, nausea, or blurred vision.
Chaotic environments: loud gyms, busy arenas, packed classrooms, bright stores.
Practical rule: If an activity causes a clear spike that doesn't settle reasonably soon, it was too much for that day.
When to start moving on purpose
After that initial relative-rest window, a patient can usually test a small amount of light activity if symptoms are stable enough to monitor. Walking and stationary cycling are common starting points. The key is that the first trial should be boringly easy.
A simple example:
Sit upright and check symptoms.
Walk slowly for a short period.
Recheck symptoms shortly after.
If symptoms rise only mildly and settle, repeat later or progress gradually another day.
If someone can't tolerate basic home activity, has severe dizziness, repeated vomiting, marked worsening, or anything else concerning, they need medical review rather than an exercise prescription.
Questions about sleep are common in this early phase because patients often think they need to stay awake or avoid normal rest entirely. Orange's guide on sleeping with a concussion is helpful for sorting out what's normal and what needs attention.
Your Evidence-Based Concussion Exercise Program
Exercise for concussion works best when it's prescribed like rehab, not like general fitness. The person needs the right modality, the right intensity, and the right progression.
The CDC's staged guidance starts with 5 to 10 minutes of light aerobic work, and it specifically notes that weight lifting should not be introduced at that stage because it can increase physiologic strain and worsen symptoms (CDC return-to-sport guidance).
Start with aerobic work, not toughness
Aerobic work is usually the anchor because it's easier to dose and easier to stop. Good first options include:
Stationary bike: often useful when head motion, balance issues, or visual motion sensitivity make walking less comfortable.
Flat walking: a good option for patients who tolerate upright movement well.
Light treadmill walking: appropriate in some supervised settings when gait and balance are steady.
What doesn't work well early is the “test yourself” mindset. Patients often try jogging, circuits, sport drills, or a gym session because they want reassurance. What they get instead is a symptom flare that muddies the rest of the day.
Add targeted rehab based on the symptom pattern
A concussion programme isn't only cardio. If the main limitation is vestibular, ocular, or cervical, the exercise plan needs to reflect that.
Examples:
Vestibular symptoms: slow head-turning tasks, graded gaze-stability work, or balance drills under clinician guidance.
Visual strain: eye-movement or visual-tracking tasks at a tolerable dose.
Neck-driven headache or dizziness: cervical mobility and stabilisation work, if assessment supports it.
A practical example is the patient who says, “Walking is fine, but supermarket aisles make me feel awful.” That's not a sign to abandon exercise. It's a sign to pair aerobic work with visual and vestibular rehab.
A sample sub-symptom progression
Stage | Activity Example | Goal | Duration |
|---|---|---|---|
Stage 1 | Easy walk or stationary bike | Reintroduce movement without a significant symptom flare | 5 to 10 minutes |
Stage 2 | Slightly longer easy aerobic session | Improve tolerance to steady, low-intensity effort | Symptom-limited |
Stage 3 | Moderate aerobic work with simple movement demands | Build tolerance before sport-specific or work-specific loads | Symptom-limited |
Stage 4 | Controlled sport-specific or task-specific movement without contact | Rehearse real-world demands safely | Symptom-limited |
Stage 5 | More complex non-contact practice or higher-demand functional activity | Prepare for full participation | Symptom-limited |
This table is a framework, not a script. A hockey player, a student, a tradesperson, and an older adult recovering from a fall won't all progress through the same tasks.
What a week might look like
One patient may start with a brief stationary bike session every day and add a small amount of time only when symptoms stay stable. Another may stay at the same duration but shift from indoor walking to outdoor walking once visual motion and balance improve.
A child returning to school may tolerate morning movement but not late-day exercise after classes. An adult working part-time may need exercise before cognitive load on some days and after it on others. Timing matters because exertion and concentration interact.
For clinicians building a more structured plan that connects assessment and rehabilitation tasks, Orange's Elevate rehabilitation and performance guide gives a useful overview of how to organise progression.
How to Monitor Symptoms and Avoid Setbacks
The hardest part of exercise for concussion isn't usually choosing the bike or the walk. It's deciding what symptom response counts as acceptable.
A lot of patients still think exercise must be completely symptom-free. That's not how current rehab is usually prescribed. Modern guidance supports subsymptom aerobic exercise after about 24 to 48 hours of rest, with the key rule that any increase should be mild and transient, not a major flare that lasts for hours (aerobic exercise therapy guidance).
Think in thresholds, not absolutes
A useful analogy is a heart-rate training zone. You're not asking the patient to do nothing, and you're not asking them to red-line. You want them in a controlled band where the activity is enough to stimulate recovery but not enough to produce a prolonged symptom escalation.
Many clinicians use a simple symptom scale before, during, and after activity. The exact number matters less than consistency. What matters is whether the patient can tell the difference between:
A mild, short-lived increase
A steady build that signals the dose is too high
A delayed crash later in the day
That pattern is more informative than a single symptom score.
Pull back when symptoms rise beyond a mild increase, when they keep climbing during the session, or when the person is still clearly worse well after the activity ends.
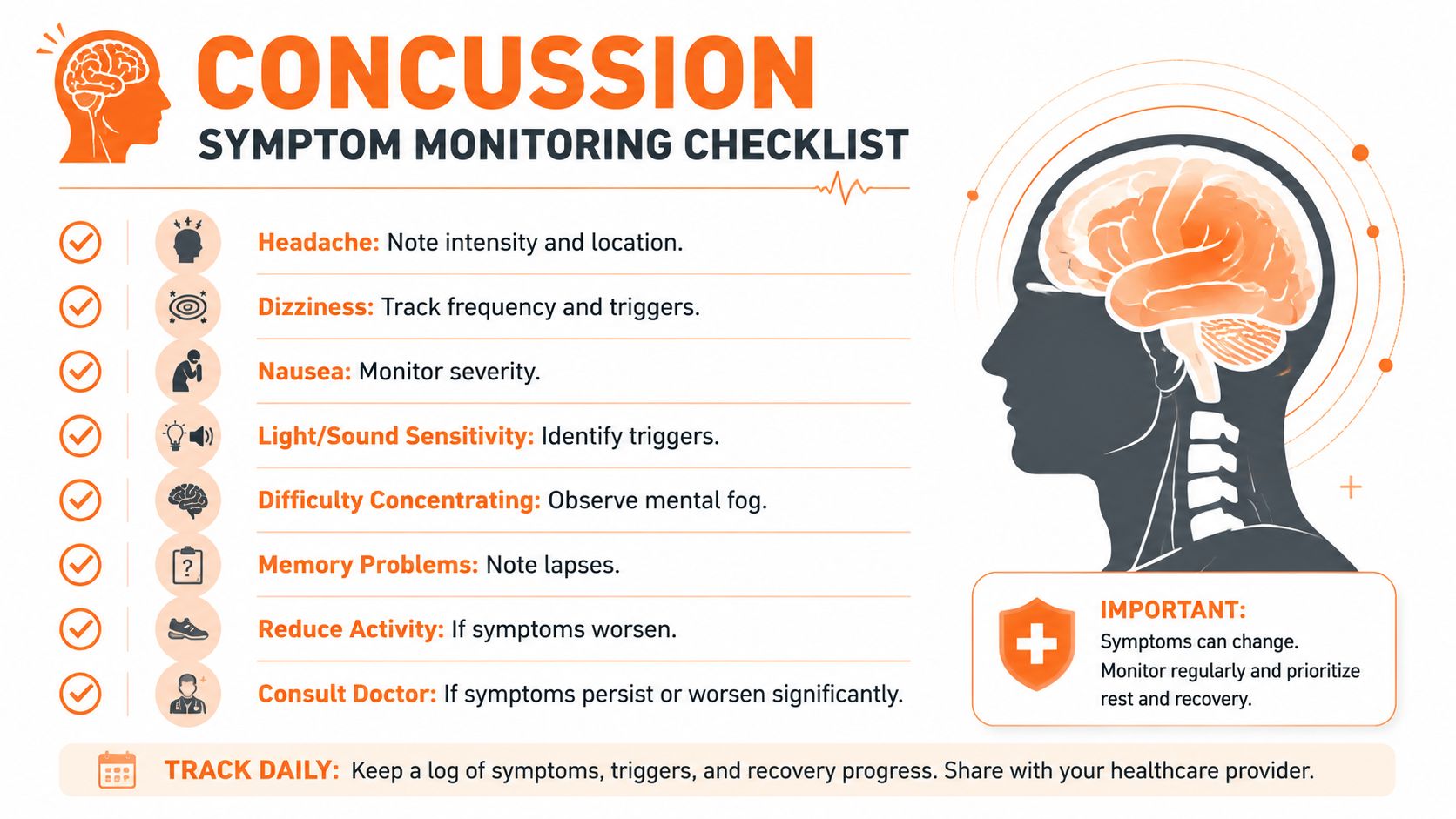
What patients should track
Good symptom monitoring is specific. “I felt bad” isn't enough to guide progression.
Ask the patient to note:
Headache pattern: Did it start immediately, build gradually, or appear later?
Dizziness trigger: Upright movement, head turns, screens, or visual motion?
Cognitive after-effect: More foggy after exertion, or clearer?
Recovery time: Did symptoms settle quickly, or linger into the evening?
Context: Sleep, school, stress, meals, and hydration can all change tolerance.
Simple logs prove very useful. A structured habit of recording duration, activity type, and symptom response gives much better clinical decisions than memory alone. For readers who want a straightforward framework for logging sessions, science-backed progress tracking can help shape the habit, even though concussion rehab needs symptom notes in addition to standard workout data.
When to stop and reassess
Some responses suggest the plan needs adjustment rather than blind persistence.
Watch for:
Symptoms that escalate quickly with minimal effort
Strong vestibular symptoms during walking or outdoor activity
Visual overload that makes upright exercise impractical
A pattern of next-day worsening after each session
In those cases, the answer usually isn't “push through.” It's to change one variable. Lower duration. Reduce speed. Switch to a bike. Separate physical work from schoolwork. Add more rest between exposures.
Patients using symptom forms often benefit from a standard measure they can repeat over time. Orange's guide to the Rivermead Post-Concussion Questionnaire is a practical reference for that process.
Personalising Recovery with Objective Assessment
Generic return-to-activity advice breaks down fast in real clinics. Two patients may both say they feel “a bit off,” yet one is mainly limited by exertion and the other by visual processing, divided attention, or vestibular strain. If you prescribe the same progression to both, one may do well and the other may stall.
That's why objective assessment matters. Symptom reports are essential, but they don't always tell you how cognition changes after exertion or whether the person's limiting factor is physical, visual, cognitive, or a mix.
Match the exercise mode to the symptom subtype
Clinical reviews have pointed out an important gap in public advice. Many articles discuss athletes returning to play but say very little about patients with visual or vestibular symptoms. For those individuals, stationary biking is often recommended over walking or running because it minimises head motion and reduces fall risk (clinical review).
That trade-off comes up constantly:
A patient with motion sensitivity may tolerate a bike but not a busy hallway walk.
A patient with neck-provoked dizziness may need cervical treatment before longer upright aerobic sessions.
A patient with visual tracking problems may report “fatigue” when the real issue is visual overload.
Use data to refine, not replace, clinical judgement
Objective digital tools are useful when they help answer practical questions. Did processing slow down after exertion? Did attention drop on school days with added activity? Does the patient recover cognitively after a lower-dose session but not after a higher-dose one?
Those answers can shape the plan:
If cognition drops after even easy aerobic work, reduce duration and retest.
If physical symptoms are mild but concentration worsens later, separate exercise from demanding cognitive tasks.
If biking is tolerated but walking in complex environments isn't, keep the aerobic dose and modify the sensory load.
One option clinicians may consider is Orange Neurosciences, which provides digital cognitive assessment and tracking across functions such as attention, memory, executive function, perception, processing speed, and eye-hand coordination. In concussion care, that kind of profiling can support decisions about pacing, school or work readiness, and whether the current exercise dose is helping or overloading the patient.
Objective measures don't remove clinical judgement. They make it easier to see whether the plan fits the person in front of you.
Baseline information also matters when available, especially in sport, schools, and recurrent injury settings. Orange's guide to baseline testing for concussion outlines how pre-injury cognitive data can support later comparison.
Your Roadmap to Full Recovery and Next Steps
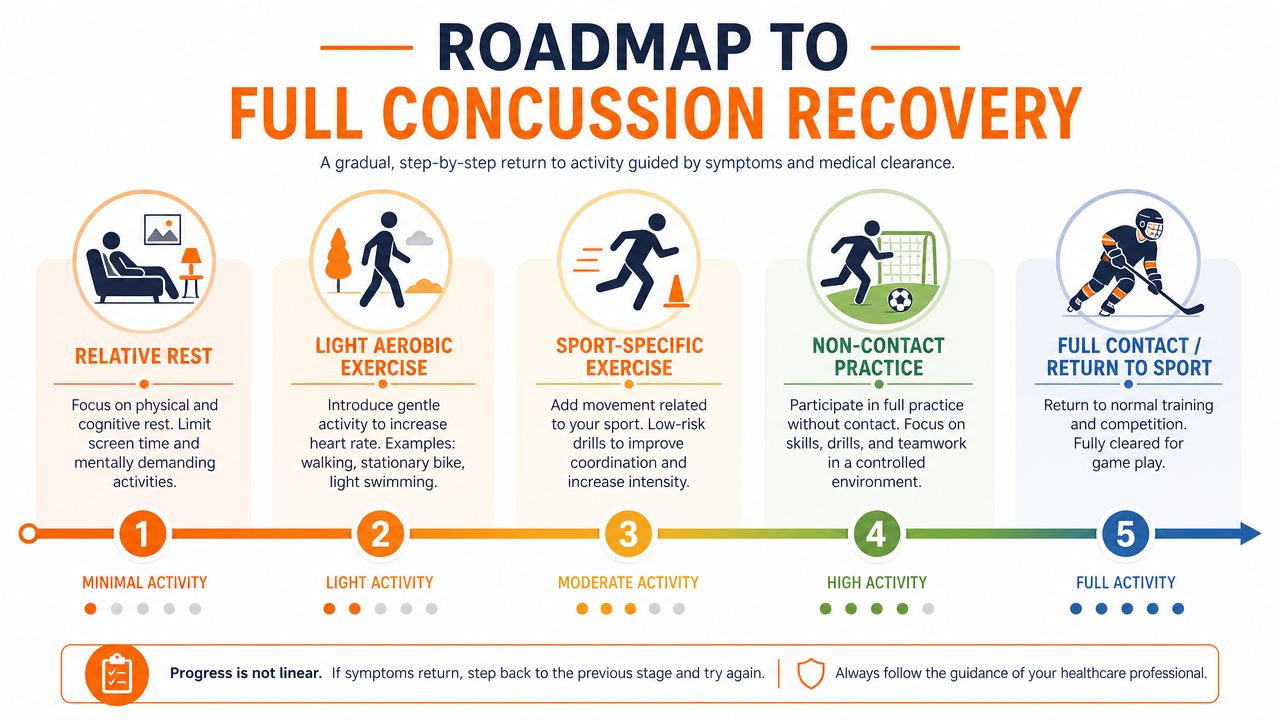
A good recovery plan is structured, but it isn't rigid. The sequence is familiar. Relative rest first. Light aerobic work next. Then more demanding movement. Then non-contact practice or work-specific tasks. Then full return when the person can handle the demands of their day or sport.
The mistake is assuming the roadmap is the same as the pace. It isn't. Some patients move through stages smoothly. Others need to pause because the barrier isn't fitness. It's dizziness, visual motion sensitivity, cognitive fatigue, neck pain, fear of symptom flare, or all of the above.
What full recovery actually requires
Returning to activity isn't just “can exercise without symptoms.” It also means the person can manage the environments and demands that matter to them.
That may include:
School tolerance: reading, screens, classes, note-taking, noise
Work tolerance: meetings, multitasking, driving, physical demands
Sport tolerance: exertion, head movement, reaction demands, contact risk
Emotional readiness: confidence, anxiety management, trust in the body again
For some patients, mental recovery needs support alongside physical rehab. If fear, frustration, or performance anxiety is becoming part of the picture, it may help to find sport psychology services that can address the behavioural side of return to play and return to performance.
The practical takeaway
Don't prescribe exercise for concussion as if it were ordinary conditioning. Dose it. Monitor it. Adjust it.
The patients who do best usually aren't the ones who rest the longest or push the hardest. They're the ones who follow a progression that fits their symptom pattern, their setting, and their actual function.
If you're a clinician, parent, therapist, or patient trying to reduce guesswork, objective cognitive tracking can make those decisions clearer. It helps connect physical progress with thinking, attention, processing speed, and day-to-day performance instead of relying on symptom descriptions alone.
If you want a more precise way to guide concussion recovery, explore Orange Neurosciences. Their platform can support clinicians and families with objective cognitive assessment data that helps personalise exercise progression, pacing, and follow-up decisions.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation