Master Your Certificate Play Therapy in 2026

You've probably had this moment already. A child sits across from you, says very little, and then tells you everything through the way they line up figures, bury objects in sand, or smash a dollhouse family apart. You know something clinically important is happening, but you also know that general counselling training doesn't always teach you how to read, structure, and respond to that process with confidence.
That's where certificate play therapy becomes more than an extra course. It becomes a way to move from “I work with children” to “I have a disciplined, supervised method for working through children's primary language of play.”
If you're newly licensed, still in graduate training, or trying to choose a credible pathway in California, the choices can feel messy. Some programmes look like weekend workshops. Others are built like a true clinical sequence. Some support credentialing. Some don't. And many clinicians are also asking a newer question: how do traditional play therapy skills fit with modern assessment tools that can help document needs and track change more clearly?
Defining Play Therapy and the Value of Certification
Think of play therapy the way you'd think about a medical specialty. A general practitioner can do excellent work across many concerns. A specialist has deeper training in one area, with a clearer framework for assessment, intervention, and decision-making.
That's the most useful way to understand play therapy. A general therapist may be warm, child-friendly, and competent with younger clients. A clinician trained in certificate play therapy learns how to use play as a structured therapeutic medium rather than as a filler activity, rapport tool, or reward at the end of session.

What play therapy actually means in practice
In ordinary child counselling, a therapist might ask direct questions, teach coping skills, or include games to keep the child engaged. In play therapy, the play itself becomes the communication channel and, in many models, the treatment process.
A simple example helps. If a seven-year-old repeatedly stages rescues, imprisonments, and sudden reversals of power with miniature figures, a trained play therapist doesn't just note that the child likes dramatic themes. They watch for patterns, pacing, emotional tolerance, symbolic meaning, and relational testing. They also know when to reflect, when to set a limit, and when not to interpret too quickly.
That difference matters because children often don't organise distress in adult language. They show it through movement, repetition, sensory choices, role assignment, and control of the play space. If you want a broader lens on why action-based learning matters for children, this hands-on learning guide for kids offers a helpful way to think about how many children process experience through doing, not just talking.
Why a certificate matters
A certificate isn't magic, and it isn't a licence by itself. What it does offer is structure.
A serious certificate pathway usually gives you:
A defined model: You're not improvising with toys. You're learning a theory-based approach.
Clinical language: You can describe what you're doing to parents, supervisors, schools, and employers.
Ethical boundaries: You learn what counts as developmentally appropriate intervention and what crosses into poorly contained practice.
Recognisable training evidence: Employers and referral partners often want to see more than “interested in play therapy.”
Practical rule: If a programme teaches techniques without a clinical model, supervision, and a clear scope of practice, it's training in activities, not training in therapy.
For clinicians in California, the evidence conversation also matters. Child-Centred Play Therapy (CCPT) is recognised in California as a promising evidence-based intervention for children ages 3 to 10 with social, emotional, behavioural, or relational difficulties. The Title IV-E Prevention Services Clearinghouse reports measurable positive effects across several child outcomes, including behavioural and emotional functioning with an overall effect size of 0.05 based on 12 studies, 30 effect sizes, and 760 children; social functioning with an effect size of 0.32 based on 5 studies, 10 effect sizes, and 280 children; and educational achievement and attainment with an effect size of 0.34 based on 5 studies, 24 effect sizes, and 228 children in its CCPT evidence summary.
If you're comparing clinical models and trying to understand how evidence and evaluation fit together more broadly, Orange also has a useful mental health assessment guide that helps frame how structured information supports treatment planning.
The Anatomy of a Certificate Play Therapy Program
When a programme is worth your time, you can usually see its structure immediately. It doesn't look like a random collection of playful interventions. It looks like a progression from theory to method to supervised application.

One California-facing benchmark is that certificate-style training often unfolds over months rather than a single short event. The University of North Texas Center for Play Therapy notes that CCPT is designated as a promising evidence-based mental health intervention by both the Title IV-E Prevention Services Clearinghouse and the California Evidence-Based Clearinghouse for Child Welfare, and it also describes an accredited therapeutic play certificate format with 15 training days delivered as 5 modules of 3 days each over 7 to 9 months, designed to help participants practise safely and effectively with children experiencing slight to moderate problems in its CCPT training overview.
The five parts of a strong programme
Most credible certificate play therapy programmes include five building blocks.
Foundations and history
You need to know where the field came from. That includes the evolution of therapeutic play, the logic behind non-directive and directive approaches, and the developmental assumptions built into each model.
Without this piece, newer clinicians often do one of two things. They become too passive and call it child-led work, or they become too controlling and call it treatment.
Theories and models
Good programmes refine the training, helping you distinguish among major orientations and understand what each one asks of you in session.
You may study areas such as:
Child-centred models: where the therapist tracks, reflects, and sets carefully bounded limits
More directive approaches: where activities are selected to support a defined therapeutic aim
Developmentally informed frameworks: where the therapist matches intervention to the child's regulation, symbolism, and capacity
You don't need to master every model at once. You do need enough exposure to know which one you are practicing.
Techniques are not the same as competence
Students often get excited about the visible tools first. Sand trays, puppets, art materials, miniature figures, storytelling prompts, and sensory objects all matter. But these aren't the heart of the training.
The heart is learning questions like these:
What does this intervention invite emotionally?
Is the child using play to express, avoid, regulate, test, or repeat?
What is the therapist's role at this exact moment?
How do I keep the work therapeutic rather than chaotic?
The toy is never the intervention by itself. The intervention is the therapist's use of timing, meaning, limit-setting, and relationship.
Ethics and professional practice
Many weaker programmes falter here, but this section is profoundly important. Work with children always includes systems around the child. Parents, caregivers, teachers, schools, and referrers all influence treatment.
A quality programme should address:
Consent and assent: Who agrees to treatment, and how do you include the child's voice?
Parent consultation: What belongs in parent feedback, and what should remain protected in the playroom?
Cultural responsiveness: How do family norms, language, migration history, and identity shape play themes and expectations?
Scope of practice: When does a child need referral, consultation, or a different level of care?
If you work in integrated care or collaborative settings, a client-centred care primer can be useful because it highlights how treatment stays anchored in the needs of the child and family rather than the provider's preferred technique.
Why supervision changes everything
Didactic learning teaches concepts. Supervision teaches judgement.
A trainee might watch a child knock down the same tower six times and conclude, “The child is dysregulated.” A supervisor may ask whether the repetition reflects mastery, invitation, aggression, testing of reliability, or a symbolic trauma sequence. That's the leap from observation to formulation.
Look closely at whether a programme includes live supervision, fieldwork, or structured review of your clinical work. If it doesn't, you may finish with vocabulary but not with durable skill.
Navigating Accreditation and Professional Credentials
Many early-career clinicians lose time assuming any play therapy certificate will move them toward recognised credentials. It won't.
Some certificates are primarily continuing education. Some are academically organised but not mapped to a credentialing pathway. The strongest programmes tell you exactly how coursework, supervision, and practica line up with professional standards.

What credential alignment actually means
When clinicians talk about the alphabet soup of the field, they're usually referring to pathways connected with the Association for Play Therapy (APT) and credentials such as Registered Play Therapist (RPT) or school-based versions of that recognition.
The practical issue isn't the letters themselves. The practical issue is whether your training counts.
A strong California example is the California State University, Sacramento Certificate in Play Therapy. Sac State describes it as a 10-unit graduate certificate explicitly designed to satisfy the APT eligibility pathway for Registered Play Therapist credentials, with coursework that includes advanced modules and supervised practice in its graduate certificate listing.
How to evaluate a programme before you enrol
Ask direct questions before paying a deposit or committing months of time.
Use this checklist:
Does the programme state its credential pathway clearly?
If the answer is vague, assume the alignment may be weak.Is supervised practice embedded?
A course that only offers lectures may be educational, but it may not support the professional outcome you want.Are the course topics competency-based?
Look for history, seminal theories, methods, diversity, special topics, and fieldwork rather than broad “working with children” language.Can you document what you completed?
You'll want clean records later for applications, credential review, or employer verification.
Supervisor's advice: Choose the programme that reduces ambiguity. The best training saves you from finding out later that your favourite elective doesn't count.
Why this matters for your career path
If your long-term goal is to work in schools, child clinics, private practice, or hospital-adjacent settings, credibility matters. Parents rarely ask for a philosophical explanation of your model. Employers don't either. They want to know whether your preparation is coherent, recognised, and transferable.
That's why credential alignment is stronger than simple course completion. It signals that someone built the training around defined competencies, not around marketing language.
For clinicians comparing child-focused modalities more broadly, a cognitive processing therapy training overview can be a useful contrast. It shows how good clinical training in any speciality becomes more valuable when the pathway is explicit, not implied.
Choosing Your Path Online vs In-Person Programs
There isn't one correct format. There is only the format that best fits how you learn, how you work, and what support you need to build confidence.
I've supervised clinicians from both routes. Some thrive online because they're disciplined, reflective, and willing to practise outside formal class hours. Others need the immediacy of room-based learning, where they can see body posture, hear tone shifts clearly, and role-play with less friction.
Where in-person training often helps most
In-person programmes tend to shine when you're learning skills that depend on subtle relational timing. That includes limit-setting, tracking, pacing, therapeutic use of silence, and the non-verbal management of intensity in the room.
If you've ever watched a live demo and immediately realised, “I wouldn't have caught that from slides,” you already understand the advantage.
In-person formats may fit you if:
You learn by watching and doing: Live modelling matters more to you than self-paced review.
You want faster feedback: Faculty and peers can respond to your posture, wording, and room presence in real time.
You struggle to separate work and study at home: Travel can create the mental boundary you need.
Where online training may be the better choice
Online programmes open doors for clinicians balancing employment, family care, or geography. They also make specialised training available to people who'd otherwise have no local access.
That flexibility isn't trivial. For many working counsellors, online delivery is the only realistic path to certificate play therapy training.
Online formats may suit you if:
You need schedule flexibility: You're fitting training around a full caseload or graduate study.
You live far from major training centres: Travel time would make in-person learning unrealistic.
You're comfortable with self-direction: You can keep up with reading, practice, and consultation between sessions.
Comparison of Online vs. In-Person Play Therapy Certificate Programs
Factor | In-Person Programs | Online Programs |
|---|---|---|
Learning experience | Strong for live role-play, observation, and immediate relational feedback | Strong for flexible access, recorded review, and wider geographic reach |
Schedule | Often requires travel and fixed attendance blocks | Often easier to fit around work and family commitments |
Practice development | Easier to rehearse room-based presence and toy-room setup in real time | Can still offer good practice, but you'll need to be intentional about skills rehearsal |
Supervision feel | Often more natural for spontaneous discussion and modelling | Can be excellent if consultation is structured and interactive |
Access | Best for those near training hubs | Best for clinicians in remote or underserved areas |
Daily cost beyond tuition | May include transport, accommodation, and time away from work | Usually lowers travel burden and may reduce disruption to your schedule |
Choose the format that makes it most likely you'll finish, practise, and integrate the model well. The “best” programme on paper isn't best if your life setup makes completion unlikely.
One more point that students often overlook: ask how each format handles supervised review of your actual work. A brilliant lecture series won't compensate for thin consultation.
The Real-World Impact of Your Play Therapy Certificate
A play therapy certificate doesn't create a new California licence. That's an important reality to understand from the start. It sharpens your speciality within the licence you already hold or are working toward.
That distinction can disappoint people at first, but it is useful. It keeps your focus on what the certificate is supposed to do: improve your competence, clarify your professional identity, and make your services more relevant to children and families who need them.
What changes professionally
In California, play therapy is a specialty technique rather than a separate licence. The broader legal authority to provide psychotherapy sits with licensed professions such as LMFTs, LPCCs, LCSWs, and psychologists, and one practical concern is whether specialist training changes employability or access. The University of North Texas notes that many California counties are designated as mental health professional shortage areas, which makes a specialised, evidence-based credential a meaningful differentiator in high-need child-serving contexts in its California-oriented certification discussion.
That translates into several real-world effects.
You become easier to place
Agencies, schools, and clinics often need clinicians who can say more than “I also see children.” A play therapy certificate gives employers a clearer picture of your niche.
It can help when you want to:
Join a child-focused practice
Support school-aged referrals with more confidence
Build a private practice identity around younger clients
Collaborate with paediatric or family-serving teams
What changes clinically
The deeper impact is in the room.
When you're properly trained, you stop treating child sessions as simplified adult sessions. You become better at reading symbolic communication, selecting developmentally matched interventions, and handling parent involvement without losing the child's therapeutic space.
Here's a grounded example. A child referred for “behaviour problems” may spend weeks in repetitive control-and-capture play. A less specialised clinician may push for verbal insight too early, redirect too often, or mistake symbolic repetition for non-compliance. A trained play therapist is more likely to recognise the protective function of the play, regulate the pace of intervention, and use the relationship itself as a treatment tool.
A certificate doesn't just add techniques. It changes what you notice, how you formulate, and what you do next.
Why access matters in California
This point deserves attention because it gets missed in promotional copy. Certificate play therapy isn't only about your CV. In shortage areas, specialised training can affect whether children get developmentally appropriate care at all.
If you're one of a small number of clinicians in a county who can work skilfully with young children, your certificate may shape referral patterns, waiting list decisions, and family follow-through. Parents often struggle to find someone who doesn't “talk at” their child. Specialised preparation helps you meet that need with a method that makes sense for children.
For newly licensed counsellors, this is the practical takeaway: your certificate won't replace licensure, but it can absolutely sharpen your role in systems that are already stretched.
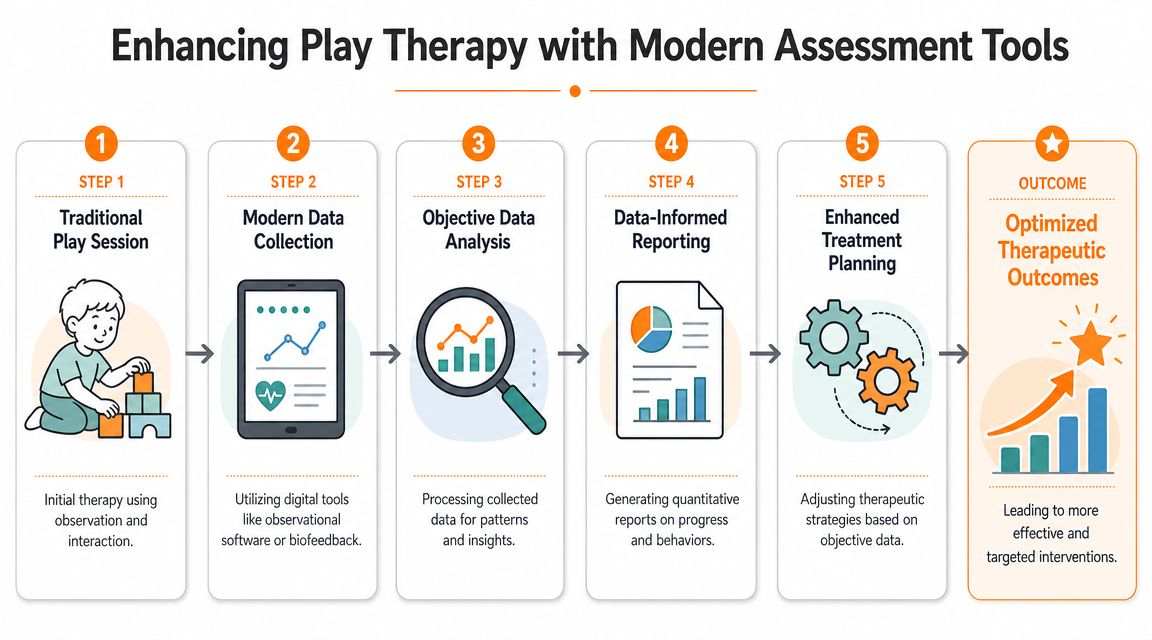
Enhancing Play Therapy with Modern Assessment Tools
Traditional play therapy relies heavily on observation, attunement, developmental understanding, and the therapeutic relationship. None of that should be replaced. But many clinicians now want better ways to document what they're seeing, communicate it clearly to families and referral sources, and track whether a child's functioning is changing over time.
That's where modern assessment tools can complement play therapy rather than compete with it.
What technology can add to your clinical picture
Suppose you notice that a child has trouble with turn-taking, loses track of multi-step play narratives, and becomes frustrated when tasks require sustained focus. In the playroom, those observations matter. They shape your pacing, your expectations, and your treatment plan.
A modern digital cognitive assessment can add another layer. It may help you gather structured information about areas such as attention, executive functioning, memory, processing speed, or eye-hand coordination. That doesn't tell you the meaning of the child's play. It does help clarify whether certain difficulties may be affecting how the child engages with therapy, school demands, or home routines.
A practical way to integrate both
A balanced workflow might look like this:
Start with clinical observation: Notice play themes, regulation patterns, relational tests, and sensory preferences.
Use structured assessment when needed: Bring in objective cognitive data if attention, planning, or processing concerns seem relevant.
Compare the two sources: Ask whether the data supports, complicates, or sharpens your original formulation.
Adjust treatment planning: You may slow instructions, simplify transitions, alter expectations for symbolic play, or recommend further evaluation.
This is especially useful when you need to explain your reasoning to caregivers. Parents often understand “your child showed these patterns in play and in structured cognitive tasks” more readily than a purely interpretive summary.
Good assessment doesn't replace therapeutic judgment. It gives that judgment cleaner edges.
If you want to explore this intersection further, Orange's cognitive assessment tools guide offers a practical overview of how digital tools can support observation, reassessment, and care planning without turning therapy into a data-only exercise.
Ethical guardrails matter
Use any tool with discipline. Assessment should support care, not overwhelm it. You still need informed consent, clear explanation of purpose, and appropriate interpretation within your professional scope.
The key is integration. Play therapy helps you understand the child's inner world and relational process. Modern assessment can help you document functional patterns with more precision. Together, they can produce a fuller, more defendable care plan.
Frequently Asked Questions About Play Therapy Certificates
Can I practise play therapy with only a certificate?
Usually, no. In California, play therapy is generally understood as a specialty technique rather than a separate licence. That means the certificate is typically an add-on to an existing professional pathway rather than a standalone right to practise psychotherapy. If you're still in training, treat the certificate as specialised preparation that sits alongside your graduate education, supervision, and eventual licensure.
Do I need a master's degree before starting certificate play therapy training?
That depends on the programme. Some are designed for licensed clinicians. Others may admit graduate students or pre-licensed professionals. The key question isn't only admission. It's whether the coursework will count toward your long-term credentialing goal and whether you'll have the clinical context to apply it responsibly.
A good rule is simple: check admission criteria, supervision requirements, and credential alignment before enrolling.
How do I know if a certificate is serious or just a short workshop?
Look for signs of structure.
A stronger programme usually includes:
A defined theory base: not just a list of activities
Supervised practice: not only lectures
A multi-month format: enough time to integrate learning
Clear documentation: so you can show exactly what you completed
Credential relevance: especially if you want an RPT-related pathway
If the programme description stays vague about supervision, competencies, or how the training fits recognised standards, slow down and ask questions.
Will a certificate make me more employable?
It can, especially if you want to work with children and families. But the effect depends on your licence, setting, referral network, and whether the training is well aligned with recognised credentials.
Think of it this way. A certificate doesn't guarantee a job. It does make your child-speciality profile clearer, and in areas where child mental health access is strained, that clarity can matter.
What if I'm interested in related child development training too?
That can be a smart move, especially if you work in interdisciplinary settings. Some clinicians pair play therapy study with coursework in school mental health, developmental assessment, or occupationally informed child support models. If you're mapping adjacent training options, this occupational therapy course guide may help you think through how child-focused disciplines overlap while still serving different clinical purposes.
The main thing is to stay strategic. Don't collect disconnected certificates. Build a pathway.
If you're building a child-focused practice and want better ways to support your clinical judgement with structured cognitive data, explore Orange Neurosciences. Their tools can help clinicians, educators, and families gather objective information that complements therapeutic observation, supports clearer care planning, and makes progress easier to track. If you'd like help thinking through how digital assessment could fit your setting, reach out through the website or email the team directly.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation