Occupational Therapy Course in Canada
Apr 25, 2026

You might be reading this because you've seen occupational therapy change someone's life up close.
Maybe a parent learned how to dress independently after a stroke. Maybe a child who struggled at school finally found tools to focus, write, and join in. Maybe you're the one considering a career shift because you want work that combines science, problem-solving, and direct human impact.
That instinct makes sense. Occupational therapy sits at the meeting point of health, function, and daily life. It isn't only about recovery in a clinic. It's about helping people return to the activities that give their day structure and meaning, from showering and cooking to handwriting, working, learning, and managing emotions.
An occupational therapy course is the training ground for that work. It teaches you how the body moves, how the brain processes information, how illness or injury disrupts everyday routines, and how to build practical interventions that help people re-engage with life. For many students, it also becomes a shift in perspective. You stop looking only at diagnosis and start looking at participation.
If you're exploring programs, changing careers, or trying to decide whether OT fits your strengths, a good starting point is this broader guide to occupational therapy in Canada. It helps place the profession in context before you compare schools and course structures.
Your Journey into Occupational Therapy Starts Here
A prospective OT student often starts with a simple observation. Someone they know is technically "better" after medical treatment, but still can't manage ordinary life. They can stand, but not cook. They can speak, but not organise a morning routine. They can go back to school, but not keep up with attention demands, handwriting, or sensory overload.
That's where occupational therapy becomes real.
I still tell students to think of OT through a practical lens. If medicine helps a person survive, OT helps them live their day again. An occupational therapist asks, "What does this person need, want, or have to do?" Then we work backward from there. That might mean improving hand strength, adapting a classroom task, redesigning a bathroom setup, or teaching a caregiver how to support independence without taking over.
Occupational therapy is one of the few professions that treats function as the outcome people feel most deeply.
An occupational therapy course reflects that same mindset. You won't only memorise anatomy terms or theories of development. You'll learn how those ideas show up in real tasks. Why does reduced shoulder movement make dressing harder? Why does slowed processing speed affect classroom performance? Why can someone score well on a basic test but still struggle to manage meals, medication, or work demands?
What students usually want to know first
Most prospective students ask practical questions before philosophical ones:
What qualification do I need? In Canada, entry-to-practice training is typically at the master's level.
What will I study? Expect human movement, neuroscience, assessment, ethics, clinical reasoning, and fieldwork.
Will I get hands-on experience? Yes. Fieldwork is a major part of OT education.
Can I specialise later? Absolutely. Many therapists move into paediatrics, neurorehabilitation, mental health, geriatrics, school-based practice, and community care.
The path can feel long when you're standing at the beginning of it. But it's much less confusing once you understand what OT education is trying to build. It isn't producing technicians who follow scripts. It's preparing clinicians who can observe, analyse, adapt, and teach in real time.
Understanding the Core of Occupational Therapy Education
Occupational therapy education makes more sense once you understand one key word: occupation.
In everyday speech, people hear that word and think "job." In OT, it means the activities that fill a person's life. Eating breakfast. Getting dressed. Managing school routines. Playing. Parenting. Returning to work. Taking transit. Joining a hobby group. Resting well enough to function the next day.
That broader meaning changes everything.
Occupation means daily life in action
I often describe an OT as a blend of life skills coach, movement analyst, and environmental problem-solver. We don't only ask whether a body part works. We ask whether the person can use their abilities in the place, routine, and role that matters to them.

A simple kitchen task shows the difference. Suppose an older adult can grip a spoon but still can't prepare lunch safely. An OT doesn't stop at grip strength. We look at sequencing, memory, balance, fatigue, vision, reach, and the kitchen setup itself. That same logic applies across age groups and settings.
If you want a helpful way to think about daily function, this guide on ADL vs IADL is useful. It breaks down the difference between basic self-care and the more complex tasks needed for independent living.
OT and OTA aren't the same role
Applicants often get mixed up at this stage.
An Occupational Therapist (OT) is trained to assess, plan, adapt, and evaluate intervention at a deeper clinical level. OTs make complex decisions about function, environment, goals, and safety. They interpret assessment findings and shape the treatment plan.
An Occupational Therapy Assistant (OTA) supports service delivery, often by helping carry out interventions and documenting what happens in practice. The exact role can vary by setting and supervision structure. The important point is that OTA education is not the same as OT education, and it does not lead to the same scope of practice.
So when you're searching for an occupational therapy course, be sure you're looking at the qualification that matches the role you want.
Why standards matter in Canada
In Canada, professional standards shape what competent entry-level practice should look like. That matters because OT is not casual helping work. It involves clinical judgement, ethics, communication, documentation, and a strong understanding of person-centred care.
A strong course teaches you to think in layers:
The person and their strengths, limits, goals, and habits
The task and what it demands physically, cognitively, and emotionally
The environment including home, school, clinic, workplace, and community
The fit between all three
Practical rule: If a program description talks only about treatment techniques and barely mentions occupation, context, or participation, look more closely. OT education should always return to real-life function.
This occupation-centred philosophy is what makes OT distinct. It also explains why the training has to be broad. You need enough science to understand impairment, enough theory to guide reasoning, and enough practical experience to turn both into meaningful change.
Navigating OT Program Levels and Accreditation
A prospective student often reaches this point with two browser tabs open. One says master's. The other says doctorate. Both promise a path into occupational therapy, and both can sound convincing until you ask the question that matters most in practice: which route prepares you for the kind of clinician you want to become?
Program level matters, but degree title alone can mislead. In Canada, the MScOT is still the route most applicants investigate first. In parts of North America, entry-level doctoral programs are also available, and analysts at Data USA's occupational therapy profile report that doctoral programs are typically longer than master's programs. That extra time often reflects added work in leadership, systems improvement, research translation, or programme development rather than a completely different clinical profession.
The simplest way to read the difference is this. Both pathways aim to prepare students for entry-to-practice OT work. The doctorate usually adds another layer, much like adding an advanced design studio to a strong clinical apprenticeship.
The master's route and the doctorate route
The Master of Science in Occupational Therapy (MScOT) usually centres on the foundations you need to start practice safely and effectively: assessment, intervention planning, clinical reasoning, professional ethics, and fieldwork. For many students, that is the right fit because it is the established path and keeps the focus close to direct client care.
An entry-level Doctorate of Occupational Therapy (OTD) commonly includes that same clinical base, then extends it into areas such as leadership, knowledge translation, service design, teaching, or innovation. This can suit a student who already sees themselves doing more than one kind of work over time, such as treating clients, helping shape programmes, or bringing new tools into practice.
Consider this comparison:
Feature | Master of Science in OT (MScOT) | Entry-Level Doctorate of OT (OTD) |
|---|---|---|
Primary purpose | Prepares students for entry-to-practice clinical work | Prepares students for entry-to-practice and often adds stronger emphasis on leadership or advanced scholarly work |
Typical length | Shorter than an entry-level doctorate in North America | Longer than a master's route in North America |
Common student fit | Students who want the established path into practice | Students interested in broader systems, innovation, research, or advanced professional development |
Curriculum feel | Strong clinical core with fieldwork and applied reasoning | Clinical core plus additional depth in projects, leadership, or advanced practice topics |
Key question to ask | Does this program's placements and teaching style fit my goals? | Does the additional time and academic depth match how I want to practise? |
For career-changers, this distinction can reduce a lot of confusion. The MScOT is often like learning to build a house well from the ground up. The OTD may include that same construction training plus added work on planning neighbourhood infrastructure, evaluating outcomes, and improving the systems around care.
Accreditation shapes what your degree can do for you
Accreditation is the checkpoint that turns a course from interesting study into a professional pathway. If your goal is to practise as an OT, you need a programme that aligns with recognised entry-level standards and supports the route to professional recognition in the place where you intend to work.
Students sometimes get distracted by the visible features of a programme. New campus. Flexible timetable. Strong marketing. Those details matter, but they sit below the first question: will this qualification be recognised for the registration pathway I need?
That question has become even more important as OT education starts to include more technology-rich learning. A strong modern programme does not add digital tools as decoration. It teaches you how to use them clinically and critically. For example, coursework that connects motor learning, neurological rehabilitation, and digital assessment can prepare you to understand tools grounded in fundamental movement skills in rehabilitation and development. That kind of training matters because future practice will increasingly involve data-informed decision-making, remote monitoring, and technology that supports participation outside the clinic, not just inside it.
Questions worth asking before you apply
Good applicants do more than meet grade requirements. They ask specific questions that reveal how a programme works.
Professional recognition: Which accrediting and regulatory expectations does this programme meet for the region where I want to practise?
Placement mix: Where do students complete fieldwork, and do those sites include hospitals, schools, community services, mental health, and neurological rehabilitation?
Teaching approach: How are theory, simulation, and clinical reasoning taught? Will I spend most of my time in lectures, case-based seminars, labs, or blended formats?
Technology in training: Does the course expose students to digital assessment tools, telehealth workflows, or rehabilitation technologies they are likely to meet in practice?
Faculty interests: Are the lecturers active clinicians, researchers, or both, and do their interests match the populations or settings I care about?
Preparation pathway: If you are entering from another profession or need a stronger academic bridge, the Access to Higher Education Diploma Health Professionals can help you build that foundation before applying.
A good programme shapes your habits of thought. It teaches you how to judge evidence, explain your choices, document clearly, and adapt when real life is messier than the textbook case.
That is why applicants should judge programmes by professional fit, recognised standards, and future relevance, not by degree label alone.
A Look Inside a Typical OT Course Curriculum
The best way to understand an occupational therapy course is to stop thinking of it as one subject. It's really a woven curriculum. Anatomy alone won't make you a therapist. Neither will theory on its own. OT training works because it connects body systems, human behaviour, environment, task demands, and clinical reasoning.
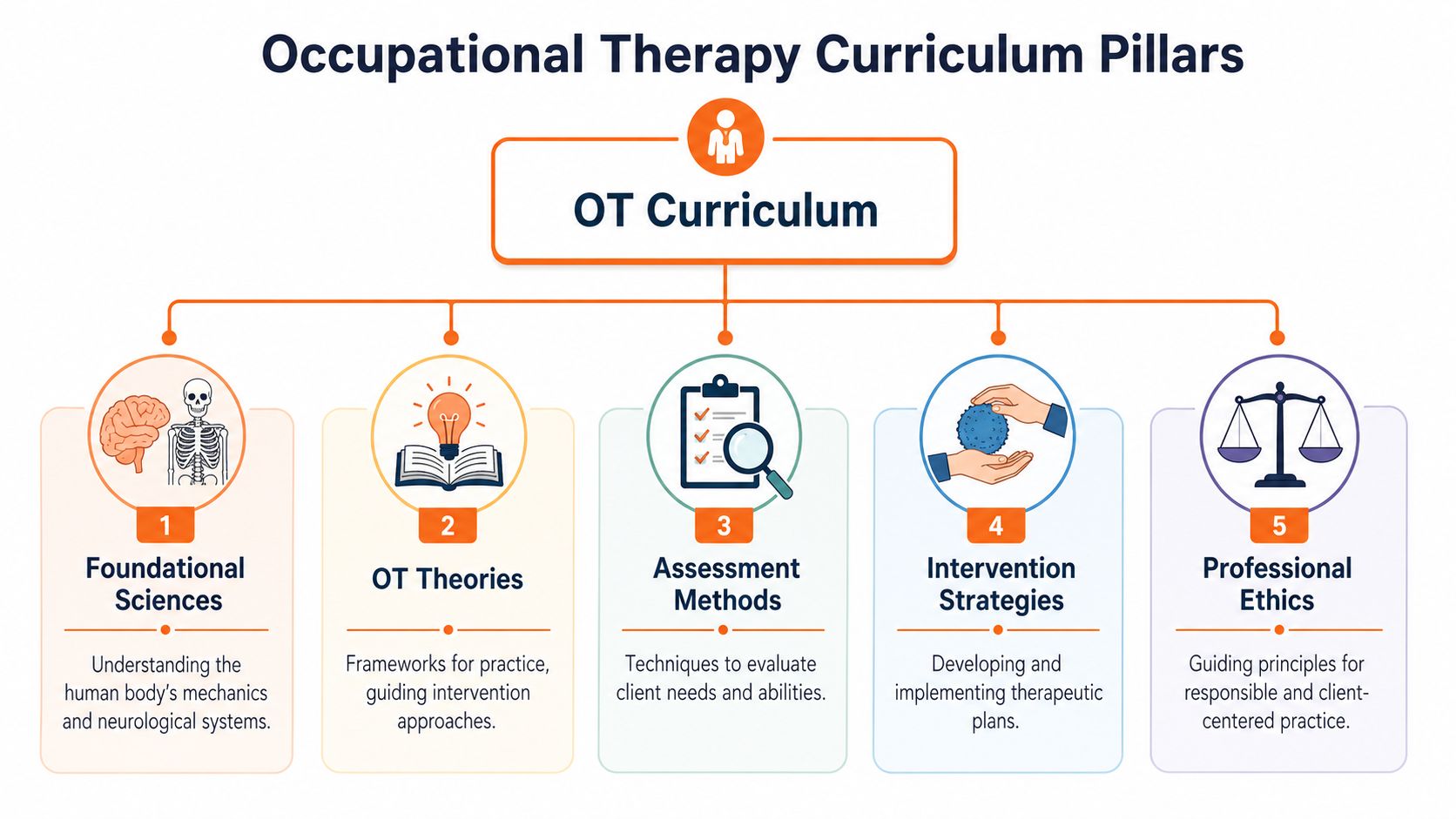
The science foundation
Early coursework usually builds a base in the sciences that explain how people move, think, sense, and adapt. Students often meet neuroanatomy, kinesiology, physiology, psychology, and human development here.
These subjects can feel abstract at first. Then the connection clicks.
A student learns the anatomy of the hand, then analyses why buttoning a shirt is difficult after injury. They study attention and executive function, then connect those ideas to school performance, medication routines, or safe cooking. They learn how postural control works, then see why a person struggles to sit upright long enough to eat independently.
OT theory and professional reasoning
Theory gives OT students a structured way to think. It helps you decide what matters, what to assess, and how to explain your intervention choices.
In practice, theory stops you from treating isolated symptoms without understanding the person's life. A client isn't only "poor balance" or "weak grip." They may be a grandparent who wants to carry a toddler safely, a student who can't manage classroom transitions, or an adult recovering from a brain injury who can't return to work routines.
A typical course asks you to justify your decisions, not just perform tasks. That habit becomes one of the most valuable parts of training.
Assessment and simulation labs
This is often where students start to feel like clinicians.
Top-tier Canadian OT courses, such as McMaster University's MSc(OT), require students to master over 15 standardised assessments and achieve interrater reliability above 90% in simulation labs. These courses also integrate AI-augmented activity analysis, enabling 25% faster care plan personalisation, with 40% of alumni entering neurorehabilitation, according to the Fundamentals of Occupational Therapy course outline.
That sounds technical. In simpler terms, students don't only learn test names. They practise using assessments consistently, interpreting results carefully, and turning findings into an action plan. If two students observe the same task, their scoring should be closely aligned. That's what reliability training is trying to build.
If you're curious about how movement skills are broken down in functional terms, this guide to fundamental movement skills is a practical companion. It shows why movement analysis matters beyond sport or exercise.
What daily learning can look like
A week in an OT programme can be varied. You might move between:
Lectures: Foundations in neuroscience, ethics, development, or models of practice
Skills labs: Transfers, activity analysis, observation, documentation, interviewing
Case work: Reviewing client scenarios and building intervention plans
Simulation: Practising assessments with peers, standardised cases, or technology-supported exercises
Good OT education keeps asking the same question in different ways. How does this knowledge help a real person do something meaningful?
Where digital tools enter the picture
Modern OT practice includes more technology than many applicants expect. Students increasingly encounter digital assessment tools, structured progress tracking, and platforms that support cognitive profiling or therapy planning.
That matters most in areas like paediatrics, neurological rehabilitation, school-based practice, and cognitive care. A student might learn traditional observation methods alongside digital tools that help organise findings on attention, memory, processing speed, or eye-hand coordination. Used well, those tools don't replace clinical judgement. They sharpen it.
That's one reason the strongest programmes feel both grounded and current. They still teach transfers, handwriting analysis, environmental adaptation, and therapeutic communication. But they also prepare students for a healthcare world that values faster, clearer, and more consistent decision-making.
The Critical Role of Clinical Fieldwork Placements
No occupational therapy course is complete without fieldwork. Through fieldwork, students stop imagining the role and start living it.
A lecture can teach you the principles of cognitive screening. A lab can teach you how to score an assessment. Fieldwork teaches you what happens when a client is tired, a family member is anxious, the hospital is noisy, and the plan that looked tidy on paper needs to change in real time.

In CAOT-accredited programmes like UBC's Master of Occupational Therapy, students complete 1000+ hours of required fieldwork, including 12 to 16 week neurological placements. This immersive training is linked to clinical competency and contributes to a 95% first-time pass rate on the NOTCE and a 27% improvement in neurological screening proficiency, according to the course description reference.
What those hours feel like in practice
Students often expect fieldwork to mean lots of observation at first and then a gradual move into treatment. That's true, but the experience is more layered than that.
In a neurorehabilitation unit, a student may begin by shadowing an OT through morning rounds, documenting mobility and self-care barriers, and watching how the therapist prioritises safety. Soon after, that same student may help set up a grooming task, practise transfer techniques, or co-lead a simple upper extremity activity under supervision.
In a school placement, the rhythm is different. The student might observe handwriting during class, speak with a teacher about regulation strategies, and adapt a desk setup or sensory routine to support participation. The pace can be fast, but the clinical thinking is just as rigorous.
If you're unfamiliar with OT evaluation in practice, this guide to assessment for occupational therapy helps connect the educational side to real clinical reasoning.
The supervision relationship matters
A strong placement educator does more than sign off on hours. They model how to think like an OT.
A good supervisor will ask things like:
What did you notice about the client's initiation?
Why did you choose that task and not another one?
Was the barrier motor, cognitive, sensory, environmental, or a mix?
How would you explain your plan to the family?
Those questions can feel demanding. That's the point. Fieldwork builds judgement under guided pressure.
Some students discover during placement that they love the exact setting they once feared. Others realise a popular area isn't the right fit for them. Both outcomes are useful.
Common challenges students face
Fieldwork is often where confidence dips before it rises.
You might struggle with documentation speed, speaking up in team meetings, or adjusting when a client doesn't respond as expected. You may know the theory and still freeze when asked to lead part of a session. That doesn't mean you're failing. It means you're moving from classroom knowledge to professional performance.
The students who grow fastest usually do three things well:
They ask specific questions instead of saying only, "I don't get it."
They reflect after each day on what worked, what didn't, and why.
They accept feedback without becoming defensive, even when it's uncomfortable.
By the end of placement, most students don't just feel more skilled. They start to sound different. Their observations get sharper. Their documentation gets cleaner. Their interventions become more intentional.
That's why fieldwork remains the part of OT education that students remember most vividly. It's where the profession stops being an idea and becomes a responsibility.
Specializations and Career Pathways After Graduation
One of the best things about occupational therapy is that graduation doesn't lock you into one narrow role. Your training gives you a broad clinical foundation, but your career can move in very different directions depending on the setting, population, and problems you want to solve.

Demand is strong. The US Bureau of Labor Statistics occupational therapist outlook projects 14% employment growth from 2024 to 2034, creating about 10,200 openings each year. The same source notes that many OTs work in hospitals (26%), private clinics (23%), and schools (19%).
Paediatrics
Paediatric OTs help children participate in the occupations of childhood. That can include play, dressing, feeding, school routines, handwriting, emotional regulation, and social participation.
A paediatric therapist might work with a child who understands classroom content but can't stay organised long enough to complete written work. Another child may struggle with eye-hand coordination, transitions, or sensory processing during group activities. In these cases, OT often combines observation, task adaptation, family coaching, and school collaboration.
For readers interested in this area, this guide to occupational therapy with autism gives a useful example of how function-focused support is applied in real life.
Neurorehabilitation and physical rehabilitation
Many students first picture OT as a therapist working with someone after stroke, brain injury, neurological illness, or orthopaedic trauma, helping them rebuild function for daily life.
The work often includes upper extremity recovery, cognitive support, visual-perceptual retraining, fatigue management, home planning, and task-specific practice. The goal isn't just movement. It's meaningful use of movement.
Digital cognitive tools are becoming more relevant in this space because neurorehab often requires structured tracking of attention, memory, processing speed, and coordination over time. Clinicians who understand both functional observation and digital measurement will be especially valuable.
Geriatrics and aging in place
Older adults often don't need abstract advice. They need practical solutions that help them remain safe and independent at home.
An OT in geriatrics may assess bathroom setup, transfers, meal routines, medication management, fatigue, and fall risk. Sometimes the best intervention is exercise and task practice. Sometimes it's environmental change. Sometimes it's helping a family realise that support can be graded rather than all-or-nothing.
For a useful non-clinical overview of housing adaptations, this article on Ergonomic Office Chairs for Therapy and Wellness Practitioners: A Guide can also spark broader thinking about seating, posture, and workspace demands that therapists often address in practice.
Mental health and community practice
OT has a long history in mental health, though some applicants don't realise it. Therapists in this area may support routines, emotional regulation, sensory strategies, executive function, role recovery, social participation, and community reintegration.
A community-based OT might help an adult re-establish structure after a mental health crisis. Another may support someone who wants to return to volunteer work, manage a household, or build sustainable coping routines. The interventions can look less visibly "medical," but the reasoning is every bit as skilled.
How careers evolve over time
Many therapists don't stay in one lane forever. A new graduate may begin in hospital rehab, then move into outpatient neuro care, school practice, programme development, teaching, private practice, or health technology.
A few common career shifts include:
Clinician to specialist: developing deeper expertise in paediatrics, neurology, hand therapy, or seating
Clinician to educator: supervising students or teaching in academic programmes
Clinician to consultant: advising schools, families, workplaces, or community organisations
Clinician to innovation roles: contributing to digital health, assessment systems, or clinical product development
OT careers tend to expand through exposure. The more settings you see, the clearer your fit becomes.
That flexibility is one reason many career-changers are drawn to the profession. You train as a generalist, but your practice can become highly specialized to the kind of impact you want to make.
Choosing Your Path and Embracing the Future of OT
Once you've decided OT feels right, the next step isn't to apply everywhere. It's to choose carefully. The right occupational therapy course won't just help you qualify. It will shape how you think, how confident you become in practice, and how prepared you are for the future of care.

What to look for in a strong programme
When advising students, I tell them to move past the glossy brochure quickly. Focus on the elements that affect your actual training.
Faculty fit: Read staff profiles. Look for people whose teaching or clinical interests line up with yours.
Placement quality: Ask where students go, what supervision looks like, and how much exposure they get to diverse populations.
Clinical reasoning focus: A strong programme teaches more than techniques. It teaches decision-making.
Technology readiness: Modern practice increasingly uses digital tools for assessment, tracking, and care planning. Your course should prepare you to work thoughtfully with them.
Learning culture: Talk to current students if you can. A supportive culture matters, especially during demanding placements.
Questions that reveal more than rankings do
A school can look impressive but still be the wrong fit. Ask practical questions that reveal the learning experience behind the marketing.
Try asking:
How are students taught to connect theory to real intervention?
What kinds of feedback do students receive during labs and placements?
How does the programme address cognitive, neurological, and community-based practice?
Are students exposed to current tools used in contemporary rehabilitation and assessment?
These questions usually lead to more honest answers than broad questions about reputation.
The profession keeps changing
OT rewards people who stay curious. Your entry-level course gives you a strong base, but it won't be the end of your learning. Practice changes. New tools appear. Documentation demands shift. Client needs become more complex.
That isn't a reason to hesitate. It's one of the profession's strengths.
A therapist working in home safety may explore resources on aging in place home modifications to better understand practical environmental adaptation conversations with clients and families. Another therapist in cognitive rehab may seek additional training in structured digital assessment tools or game-based therapeutic approaches. Lifelong learning isn't extra in OT. It's part of being competent.
Why the future of OT is still deeply human
Some applicants worry that more technology means less human care. In good practice, the opposite is true.
The future of OT isn't about handing judgement to software. It's about using better tools to reduce guesswork, identify patterns faster, personalise intervention more clearly, and spend more clinical energy on interpretation, coaching, and relationship-centred care. In cognitive and neurological practice especially, therapists who can combine observation, functional analysis, and ethical use of digital tools will be well positioned.
That matters whether you're working with a child who struggles with attention in school, an adult recovering from brain injury, or an older person trying to stay independent at home. The core question stays the same: what will help this person function better in daily life?
If that question keeps pulling you back, OT may be the right profession for you. And if you're the kind of student who wants to work where rehabilitation, cognition, and modern tools meet, keep following that thread. It will likely shape the most interesting part of your career.
If you're curious about where occupational therapy is heading next, visit Orange Neurosciences. You'll see how rapid cognitive assessment, targeted therapy tools, and workflow-friendly digital support are helping clinicians, educators, and families make more informed decisions in brain health and rehabilitation.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation