Your Essential Guide to the Trail Making Test
Mar 5, 2026

The trail making test is a cornerstone of neuropsychological assessment, designed to give us a surprisingly deep look into visual attention, processing speed, and what we call executive functioning. It’s broken down into two distinct parts: Part A, a simple task of connecting numbered dots, and Part B, which asks the brain to juggle both numbers and letters.
What Is the Trail Making Test and Why Does It Matter?
Imagine you're handed two connect-the-dots puzzles, the kind you might have done as a child.
The first puzzle is straightforward. It's a sheet of paper with circles numbered 1 to 25, and your job is to draw a line connecting them in the correct sequence. This is the essence of the Trail Making Test Part A (TMT-A). It’s a clean measure of your brain’s visual scanning abilities and raw processing speed. A practical way to think of it is like sorting a deck of cards by number—a direct, linear task.
Now for the second puzzle. This one is a bit more of a mental workout. The circles contain both numbers (1-13) and letters (A-L). Your task is to alternate between them, drawing a line from 1 to A, then from A to 2, then 2 to B, and so on (1-A-2-B-3-C…). This is TMT-B, and it asks a lot more of your brain. You have to keep the complex sequence in mind, switch between two different sets of rules, and fight the automatic urge to just connect the numbers. Think of this as sorting a deck of cards by alternating between red and black cards—it requires constant mental shifting.
The Power of a Simple Path
While both parts look simple on the surface, the difference in how a person performs on each one gives clinicians a powerful window into their cognitive health.
TMT Part A: Think of this as your brain driving down a familiar, straight highway. The time it takes you mainly reflects how quickly you can process visual information and carry out a simple, pre-learned plan. A slow time might point to a general slowdown in processing, but it doesn’t give us the full picture.
TMT Part B: This is more like navigating a busy city centre during rush hour, with multiple traffic lights, one-way streets, and pedestrians. To do it well, you need cognitive flexibility—the ability to mentally shift gears—and solid executive control to manage the more complicated rules. When someone is disproportionately slow on Part B, it often signals a specific challenge with these higher-level brain functions.
For instance, a client might finish Part A in a perfectly normal 30 seconds but then take 120 seconds to complete Part B. This wide gap tells us the problem isn't just about general processing speed; it’s a specific hiccup in their ability to mentally switch tasks, which is a classic sign of executive dysfunction. This insight is immediately actionable, suggesting further investigation into executive functions is needed.
The real clinical insight from the Trail Making Test doesn't come from the raw scores alone. It's the comparison between Part A and Part B that helps us untangle a general cognitive slowdown from a more specific deficit in executive function.
This simple, pen-and-paper test has been a staple of cognitive evaluation for over 80 years for this very reason. It provides a quick and reliable snapshot of brain functions that are vital for everyday life—things like planning your day, solving unexpected problems, and tuning out distractions.
Understanding how the TMT works is the first step toward using its data to build a clear clinical picture, which is the foundation of any good neuropsychological assessment.
Administering and Scoring the TMT Accurately
The real value of the Trail Making Test comes down to one thing: precise, consistent administration. Think of it like a carefully controlled experiment in a lab. If your method changes even slightly from one person to the next, you risk collecting unreliable data. A repeatable protocol is your best defence for generating actionable insights.
It all starts with the environment. You need a quiet, well-lit room without any distractions. A ringing phone, a nearby conversation, or even a cluttered desk can split a person's focus and tack precious seconds onto their completion time. The goal is to create a setting where the only challenge is the test itself.
Setting the Stage for Success
Before you even think about starting the timer, make sure the person is seated comfortably at a table or desk. The surface should be clear and stable, and the test sheet needs to be placed directly in front of them, aligned with their body’s centre. It's a small detail, but it prevents any physical awkwardness from clouding their performance.
Standardized instructions are completely non-negotiable. For the results to be reliable, you must say the exact same thing to every single person, every single time. This is how you ensure you're comparing apples to apples across assessments.
For TMT Part A: Place the sample sheet in front of the individual. Say: "On this page are some numbers. Begin at number 1 and draw a line from 1 to 2, 2 to 3, 3 to 4, and so on, in order, until you reach the end. Do not lift your pen (or pencil) from the paper. Work as quickly and accurately as you can. Ready, begin." If they make an error on this sample, correct them immediately and confirm they understand before you proceed.
For TMT Part B: Now, present the Part B sample. Say: "On this page are some numbers and letters. Begin at number 1 and draw a line from 1 to A, then from A to 2, then from 2 to B, and so on, in order, until you reach the end. Remember to switch back and forth between numbers and letters. Work as quickly and accurately as you can. Ready, begin." Just like before, correct any mistakes on the sample.
This diagram helps illustrate the fundamental difference between the two parts of the test.
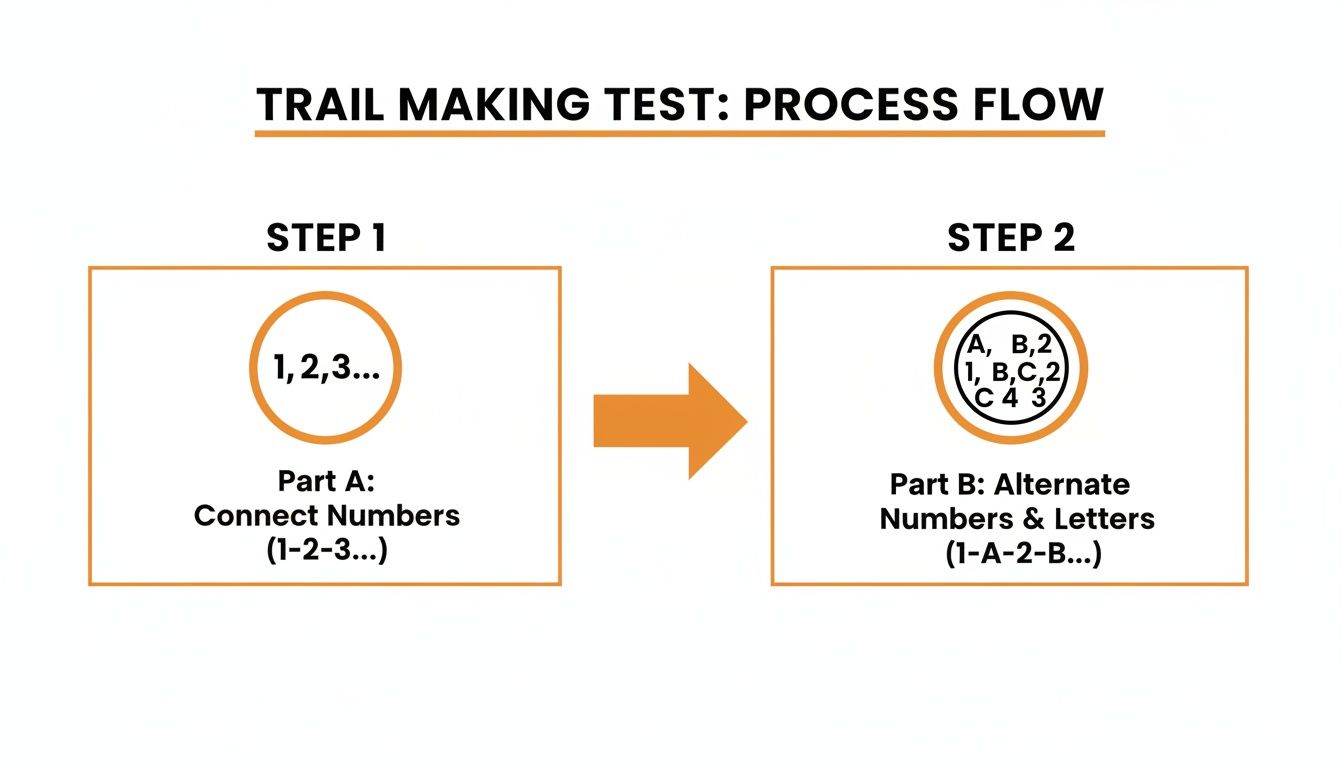
You can see how Part B isn’t just about speed—it introduces a crucial task-switching demand. This is the key that unlocks insights into executive function.
From Timing to Insightful Metrics
Scoring the TMT is so much more than just hitting 'stop' on a watch. While the time to complete each part is your primary data point, the real clinical insights emerge when you analyze the relationship between the two scores. Start your timer the moment you say "begin" and stop it as soon as the person lifts their pen or pencil after connecting the final circle.
What if someone makes a mistake but catches it and self-corrects? Don't stop the timer. The time they take to notice and fix that error is incredibly valuable clinical information. Simply record the total time for both Part A and Part B in seconds.
The most crucial step is calculating the derived scores. These are the numbers that help us see past a simple processing slowdown and spot a genuine deficit in cognitive flexibility.
Here's a quick look at the primary scoring metrics and what they can tell you.
TMT Scoring Metrics at a Glance
Score Type | Calculation | Primary Cognitive Function Measured |
|---|---|---|
Part A Time | Total seconds to complete Part A | Visual scanning, motor speed, and simple sequencing |
Part B Time | Total seconds to complete Part B | Cognitive flexibility, task-switching, and working memory |
Difference Score | B - A | Isolates the time cost of executive functioning demands |
Ratio Score | B / A | Measures the proportional increase in difficulty from A to B |
The two most powerful scores are the difference and the ratio.
Difference Score (B - A): This one is simple. Just subtract the Part A time from the Part B time. This score helps isolate the "cost" of the executive function demands in Part B. A large difference points toward a specific problem with task-switching, not just overall slowness.
Ratio Score (B / A): Here, you divide the Part B time by the Part A time. This gives you a proportional look at the cognitive load. For instance, a ratio of 2.5 means it took the person two and a half times longer to complete the more complex task.
Practical example: Imagine a person with a hand tremor who is slow on both parts (A = 60s, B = 110s). Their B-A score is 50. Now consider another person with no motor issues who scores A = 25s and B = 75s. Their B-A score is also 50, but their B/A ratio is 3.0—a clear, actionable signal of an executive function issue, prompting further investigation into cognitive flexibility rather than motor speed.
Understanding these nuances is what turns raw data into a clear picture of a person's cognitive profile. It's just as vital as ensuring strong test-retest reliability when you need to track changes over time. Of course, modern digital platforms can automate this entire process, from administration to scoring and analysis, freeing you up to focus on the person sitting in front of you. To see how, visit our website or send us an email to learn more.
Turning TMT Scores into Clinical Insights

The raw numbers from a trail making test—say, 45 seconds for Part A and 110 for Part B—are just data points on their own. Their true clinical meaning only comes to life when you put them into context. This is where normative data becomes your most powerful tool.
Think of it like this: normative data lets you compare an individual’s performance to a large, representative group of their peers. It helps you ask the right question: "How does this 70-year-old with a high school education perform compared to other 70-year-olds with similar schooling?" Without that yardstick, a score is just a number in a vacuum.
The Critical Role of Age and Education
When interpreting the TMT, age and education are two of the most significant factors you have to consider. It’s completely normal for cognitive processing to slow as we get older, so you’d expect a senior to take longer than a young adult. But the influence of education is just as profound, and it’s something clinicians can’t afford to overlook.
Practical example: A score of 100 seconds on TMT-B might be perfectly average for a 75-year-old who finished school after grade 10. But for a 40-year-old with a university degree, that very same score could be a major red flag, pointing toward a potential problem with their executive function. This insight allows you to tailor your next steps: for the older individual, you might move on to other assessments, but for the younger one, you would immediately probe deeper into executive functioning.
Why? Higher education often hones the exact skills the TMT measures: mental organization, abstract thinking, and paying close attention. If you ignore education, you risk making a serious misinterpretation—either over-diagnosing impairment in someone with less schooling or missing subtle deficits in a highly educated person.
This isn't just a theory; it's backed by hard data. Research from the California Collaborative Normative Aging Study powerfully highlighted this reality. Among 1,913 urban elders, TMT-A completion times fell by 33% as education rose from less than 12 years to over 16. The difference for TMT-B was even more staggering: a 129% gap between low-education groups and college graduates. This is precisely why personalized, education-adjusted norms—like those built into Orange Neurosciences' platforms—are so vital for an accurate assessment.
Using Percentiles to Communicate Performance
Once you compare a raw score to the right normative data, you can convert it into a percentile rank. This is one of the clearest and most effective ways to talk about performance with patients, their families, and other clinicians.
A percentile rank simply tells you what percentage of the peer group scored lower than the individual.
50th Percentile: This is right in the middle—squarely average. The person performed better than 50% of their peers.
16th Percentile: This is considered low average, sitting one standard deviation below the mean.
2nd Percentile: This is significantly below average and often suggests impairment, pointing to a notable deficit.
A percentile rank transforms a simple time score into a clear, relatable measure of cognitive standing. It shifts the conversation from "You took 95 seconds" to "Your performance was in the average range for someone your age and background."
This method is a core part of interpreting many cognitive tests. For a closer look at how percentiles are used in other key assessments, you can check out our guide on MoCA score interpretation.
Moving Beyond the Stopwatch
Ultimately, making sense of the trail making test is about connecting the dots. It’s so much more than just looking at the final time on a stopwatch. You have to consider the person's demographic background, observe their behaviour during the test, and analyze the pattern of their scores (like the B-A difference).
Did they make a lot of errors? Did they catch and correct them? Were they impulsive, or were they overly cautious and hesitant? These qualitative observations, when combined with a robust, norm-based quantitative analysis, are what allow you to build a truly insightful clinical picture. It’s this holistic approach that leads to sound clinical judgments and, most importantly, more effective care for your patients. Ready to put these insights into practice? Visit our website or email our team to learn how our tools can help.
Where the TMT Really Shines: Clinical Applications
While the numbers and ratios are fascinating, the real power of the Trail Making Test comes alive when you see it in action with actual patients. It’s one thing to have a score on paper; it’s another to see how that score helps you understand what’s happening inside someone’s head and what to do next.
Think of it as a diagnostic spotlight. For one person, it might uncover a stubborn issue after a concussion. For another, it could be the first concrete clue pointing toward a neurodegenerative disease. This is where abstract data becomes a clear path forward.
Uncovering Lingering Post-Concussion Symptoms
After a mild traumatic brain injury (mTBI), or concussion, physical symptoms like headaches often fade long before the cognitive ones. It’s common for a patient to say they “feel fine” but find themselves struggling with focus and juggling tasks at work or school. The TMT is fantastic at catching this subtle disconnect.
A classic pattern we see in post-concussion recovery is a fairly normal score on TMT-A, but a much, much slower time on TMT-B. That gap between the two parts points straight to a lingering problem with executive function, even when other symptoms seem to have vanished.
Actionable Insight Example: Imagine a 22-year-old university student who took a hit in a hockey game. He feels ready to get back to his studies and says his memory is fine. His TMT-A score is 35 seconds (average), but his TMT-B time balloons to 115 seconds (impaired). This single result gives you objective proof that his brain is still struggling with the mental flexibility needed for complex classes. This data is actionable: you can now recommend a gradual, supported return to his studies, providing clear evidence to the university's academic support office.
Early Clues in Neurodegenerative Conditions
When you suspect early-stage Alzheimer's or another dementia, a poor TMT-B score can often show up before major memory problems become obvious. Since executive dysfunction is a central part of many neurodegenerative diseases, the TMT is very sensitive to these early shifts.
For a clinician, this gives you an early, objective flag. It helps you tell the difference between normal, age-related slowing and something more clinically significant that needs a closer look.
A slow TMT-B can be an early warning flare, highlighting potential executive dysfunction that might be completely missed in a standard clinical chat focused only on memory.
Catching this early is everything. It allows for timely interventions and helps families plan for the future. For professionals looking to sharpen these diagnostic skills, enrolling in specialized clinical assessment courses can offer a much deeper understanding of how to interpret tests like the TMT in complex situations.
Charting the Course for Stroke Recovery
After a stroke, a patient's cognitive recovery is every bit as important as their physical rehab. The Trail Making Test gives us a simple, repeatable way to measure how much their attention and executive function are improving over time. By giving the test at regular points—say, at intake, one month post-stroke, and again at three months—you can create a clear data-driven story of that patient's journey.
This information is gold for shaping rehab strategies and making smarter care decisions. For example, healthcare providers using digital platforms like Orange Neurosciences' OrangeCheck see the TMT's impact firsthand. Data from a 2022 study on stroke rehab patients revealed that those who took more than 120 seconds on TMT-B had a 3.2 times higher risk of ongoing attention problems, which could stall their discharge. You can find more research on how neuropsychiatrists use TMT data to improve diagnostic speed and read about findings related to cognitive screening in senior care.
If you want to go deeper into how this specific cognitive area is assessed, you might find our guide on how to test for executive dysfunction helpful. By using tools like the TMT, we can stop guessing and start using solid evidence to guide our patients toward more targeted and effective care.
Limitations and How to Use the TMT Responsibly
A powerful tool is only as good as the person using it. While the trail making test is a fantastic resource, knowing its boundaries is key to using it ethically and getting an accurate picture of a person's cognitive health. It's a common mistake to see a slow completion time and jump to the conclusion of cognitive decline.
The truth is, many non-cognitive factors can throw off the results and lead to the wrong interpretation.
Think of the TMT as a sensitive smoke alarm. It's brilliant at telling you that there might be a fire, but it can't tell you what started it or where it is. A slow score might point to an issue with executive function, sure, but it could also be a false alarm triggered by something else entirely.
What Else Could Be Affecting TMT Scores?
Before you can interpret a slow time as a sign of cognitive trouble, you have to play detective. A good clinician knows to investigate and rule out other influences first.
Some of the most common factors that can muddy the waters include:
Motor Control Issues: Practical example: a patient with Parkinson's disease will naturally take longer to draw lines due to tremors and motor slowing, which inflates their TMT time regardless of their cognitive state.
Poor Eyesight: If someone can't see the circles clearly, their visual scanning speed will suffer. It's a simple physical limitation, not a cognitive one.
Cultural and Educational Background: The test assumes a certain familiarity with the Latin alphabet and timed tests. For someone without that background, the test itself is a learning curve, which has nothing to do with their cognitive health.
Actionable Insight: Always screen for motor and visual issues before administering the TMT. A responsible clinician never relies on the Trail Making Test alone, but uses it as one piece of a comprehensive puzzle to get a balanced view of the whole person.
The Nuance of Demographic Factors
Even things like a person's gender and education level can add another layer of complexity. For instance, data from the Halstead-Reitan California Normative Battery didn't show major gender differences overall, but a closer look told a different story. In the 70-79 age group, females were 18% slower than males on ratio scores. Why? That same group also happened to have 12% lower average education.
You can read more about how these nuances in TMT performance offer critical insights into providing fair and equitable cognitive care.
It all comes back to one crucial point: context is everything. To chalk up a slow score to cognitive decline without considering these other factors isn't just a mistake; it's a clinical misstep. The TMT is a starting point, not the final word. It's a valuable clue that tells you where you need to dig deeper, guiding you toward other tests to get the full picture.
Ready to see how modern platforms can help you navigate these complexities with automated scoring and robust normative data? Visit our website or email us to discover how Orange Neurosciences is making precise cognitive assessment more accessible.
The Future of the TMT Is Digital

It’s time to move your assessment workflow beyond the stopwatch and paper. While the traditional trail making test has been a reliable part of cognitive evaluation for decades, digital administration offers a level of precision and efficiency that pen and paper simply can't match. This shift does more than just reduce administrative burdens—it opens the door to much deeper clinical insights.
Imagine running a full TMT assessment where the timing is captured with millisecond accuracy, scores are calculated instantly, and a complete analysis is ready in moments. This is the reality with digital platforms. They practically eliminate the chance of human error in timing or scoring, a common pitfall with manual administration.
For busy clinicians, this efficiency is a true game-changer. It slashes the time spent on administrative tasks, freeing you up to focus on what matters most: your patient.
Precision and Deeper Insights
One of the biggest wins of going digital is gaining access to vast, constantly updated normative databases. We all know that traditional paper norms can become outdated. Digital systems, on the other hand, are frequently updated to reflect current population data, ensuring your interpretations are as sharp and relevant as possible.
This means you can compare a patient’s performance not just against broad age groups, but against finely tuned demographics. This leads to more accurate and reliable clinical judgements.
Practical example: A digital platform can instantly show you how a patient’s B/A ratio of 2.8 compares to thousands of their peers. It can provide a percentile rank and flag it as a potential concern in seconds, saving you the time of manually cross-referencing paper charts and tables. This actionable alert prompts you to immediately investigate further, without wasting time on manual calculations.
Building a Complete Cognitive Profile
Digital tools also allow you to integrate TMT data into a broader cognitive profile effortlessly. Instead of juggling separate scores from different tests, you can see how performance on the trail making test relates to measures of memory, attention, and processing speed, all in one unified dashboard.
A digital profile provides a complete picture of cognitive health, revealing patterns and connections that might be missed when looking at test scores in isolation. This allows for a more rounded and person-centred approach to care.
For instance, a platform like Orange Neurosciences can correlate a slow TMT-B score with a specific deficit in sustained attention measured by another task in its battery. This integrated data gives you a much more powerful foundation for your clinical decision-making.
For clinicians looking to understand how different assessments fit together, learning about other online cognitive assessment tools can be very beneficial.
Ultimately, embracing digital TMT administration means achieving better outcomes with greater efficiency. It allows you to spend less time on paperwork and more time building rapport with your patients, confident that the data guiding you is precise, current, and thoroughly analyzed. Contact us via our website to learn how you can make this transition.
Answering Your Questions About the Trail Making Test
Even seasoned clinicians run into practical questions when using the Trail Making Test. Let's walk through some of the most common situations you'll face in your practice and how to handle them with actionable insights.
What Should I Do If a Patient Has a Motor Impairment?
This is a fantastic question because it gets to the heart of what the TMT actually measures. If your patient has a significant hand tremor, partial paralysis, or even severe arthritis, their score is going to be muddied by that physical challenge.
Actionable Insight: In these situations, the TMT simply can’t give you a clean read on executive function. The best course of action is to switch to a non-motor alternative like a verbal fluency task (e.g., "Name as many animals as you can in 60 seconds") or the Stroop Test. Most importantly, make a clear note in your report explaining why you made the substitution to ensure the clinical record is accurate.
Can the Trail Making Test Be Used with Children?
Absolutely, but you have to be very careful to use a version made specifically for kids. The standard TMT you'd use with an adult is normed for an adult brain. For children and adolescents, you need a pediatric version like the Comprehensive Trail Making Test (CTMT).
Practical example: you wouldn't use an adult-sized blood pressure cuff on a toddler. Using an adult-normed test on a child will give you meaningless data. Age-appropriate norms are non-negotiable for accurately assessing conditions like ADHD, learning disabilities, or brain injuries in younger clients.
Modern digital tools, including those from Orange Neurosciences, often simplify this by including child-friendly interfaces and the correct pediatric norms right in the platform, taking the guesswork out of your hands.
How Long Should I Wait Between Tests to Avoid Practice Effects?
Practice effects are a real thing. Patients almost always get a little faster the second time they see a test, just from familiarity. To get a true sense of change, the standard recommendation is to wait at least six months between tests for routine follow-ups.
Actionable Insight: Clinical reality sometimes gets in the way. If you're tracking recovery after a stroke, you might need to test more often. If you have to re-test sooner, try to use an alternate form if one is available. No matter the time gap, always mention the possibility of practice effects in your summary to provide proper context and avoid misinterpreting a small improvement as significant clinical change.
The Trail Making Test is a staple in cognitive assessment for a reason, but its power comes from smart administration and thoughtful interpretation. At Orange Neurosciences, we've built a platform that helps clinicians do just that, with automated scoring and solid normative data to back up your clinical judgment. See how our tools can bring more clarity and actionable insights to your assessments by visiting us at https://orangeneurosciences.ca or emailing our team today.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation