Spatial Abilities Test: Unlock Your Cognitive Potential
Apr 7, 2026

A child is staring at a simple block puzzle. They are bright, talkative, and curious, yet they freeze when asked to turn a piece and fit it into place. In another setting, an older adult recovering from stroke can speak well and remember names, but keeps misjudging doorways, reaches past objects, or feels disoriented in familiar rooms.
Professionals see moments like these every day. Parents see them at the kitchen table. Teachers notice them during maths, handwriting, and construction tasks. Therapists notice them in dressing, mobility, and navigation.
These moments often point to spatial cognition. A spatial abilities test helps us look at how a person perceives shape, position, movement, and the way parts fit into a whole. That matters far beyond employment screening. It can clarify why a student struggles in geometry, why a patient finds daily tasks unexpectedly hard, or why someone with strong language still finds visual problem-solving exhausting.
The Hidden World of Spatial Skills
A child may read well, speak clearly, and still struggle to copy shapes, line up numbers, or complete a puzzle. Adults can show a similar pattern. Someone may remember instructions perfectly but have trouble parking, packing, navigating, or assembling simple items.
That gap confuses families because the difficulty does not always look like a “thinking” problem. It often looks like clumsiness, carelessness, low confidence, or poor effort. In practice, it may reflect a weakness in spatial processing.

Spatial skill is what lets a child rotate a puzzle piece in mind before moving it. It helps a teen understand how a graph changes when axes shift. It helps a stroke survivor judge where their body is in relation to a chair, a hallway, or a staircase.
What people often miss
A spatial difficulty can hide inside ordinary complaints:
“They hate jigsaws and building toys.” This may reflect trouble mentally rotating or assembling forms.
“She understands the lesson, but her geometry marks drop.” The barrier may be visual-spatial, not motivation.
“He gets lost in familiar spaces after rehab.” Orientation and spatial mapping may need direct assessment.
“Their handwriting is messy and spacing is odd.” Visual-motor and spatial planning may be involved.
For a helpful plain-language overview of this broader concept, Orange Neurosciences has a guide on spatial awareness meaning.
Clinical takeaway: When verbal ability is stronger than visual-spatial performance, daily struggles can be real even if conversation sounds completely typical.
A spatial abilities test gives us another window into function. It does not replace broader assessment. It adds a layer that many standard verbal-heavy tools miss. In schools, that can reveal hidden talent or hidden need. In clinics, it can sharpen intervention planning. In family discussions, it often replaces blame with understanding.
Understanding Your Brains GPS System
When I explain spatial cognition, I often compare it to a brain-based GPS. Not a device that speaks directions aloud, but an internal system that helps us know where things are, how they relate to each other, and what will happen if we move them.
This mental GPS supports much more than navigation. It helps with maths, drawing, dressing, driving, sports, tool use, handwriting, and many rehabilitation tasks.

Visualisation
Spatial visualisation is the ability to imagine how something would look if it changed shape, turned, folded, or unfolded.
A child uses it when thinking, “If I turn this triangle, will it fit?” A student uses it in chemistry or geometry. An adult uses it while packing a suitcase or rearranging furniture before lifting a thing.
A comparative international study found that spatial visualisation was the strongest performing spatial subscale for U.S. students, and the same paper reported development of a 27-item spatial ability test for 456 university students with high validity and reliability, supporting its use in education-focused assessment (EJ1393205).
If you work with working memory and visual processing together, the idea connects closely to the visual-spatial sketchpad.
Orientation
Spatial orientation is different. It answers, “Where am I in relation to the world around me?”
This is the skill behind following a route through a hospital, knowing left from right under pressure, or turning your body to approach a chair safely. After neurological injury, orientation problems can make a familiar room feel unpredictable.
A practical example helps. Two patients may both understand the instruction “turn and sit.” One does it smoothly. The other hesitates, over-rotates, reaches behind the chair, and sits awkwardly. The difference is not necessarily comprehension. It may be orientation.
Relations
Spatial relations concern how parts fit together and how objects are arranged relative to each other.
This appears in:
Construction tasks such as blocks, models, or assembly kits
Written work such as keeping numbers in columns
Movement tasks such as catching a ball or stepping around obstacles
Daily living such as loading a dishwasher or organising a shelf
Why the distinction matters
Professionals sometimes use “spatial” as one broad label. That can blur important differences.
Sub-skill | Everyday example | Common point of confusion |
|---|---|---|
Visualisation | Folding a box in your mind | Mistaken for general intelligence |
Orientation | Finding your way through a new building | Mistaken for inattention |
Relations | Seeing how parts fit into a whole | Mistaken for poor effort |
A person can be strong in one area and weak in another. That is exactly why a spatial abilities test can be so useful. It can move us from a vague impression, such as “not good with visual tasks,” to a more precise picture of what the person finds hard.
A Look Inside the Spatial Abilities Test Toolbox
Not all spatial tasks measure the same thing. A well-chosen spatial abilities test uses item types that target different sub-skills. For clinicians and educators, it helps to recognise the major formats on sight.
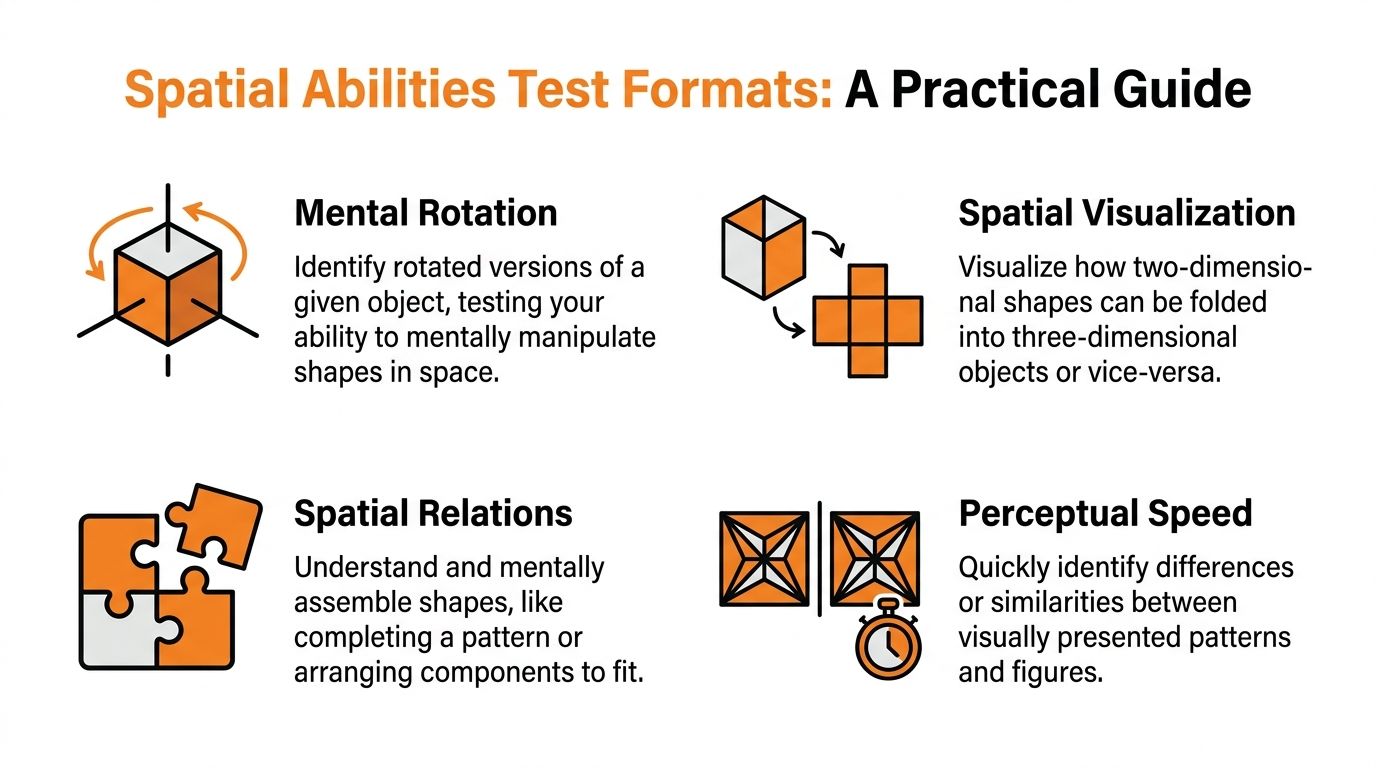
Mental rotation
Mental rotation items ask a person to identify which option matches a target shape after it has been turned.
This sounds simple until you watch someone do it. Strong performers often seem to rotate the object “in the mind’s eye.” Others compare piece by piece, lose track, or confuse a rotated figure with a mirrored one.
You see this skill in everyday situations when someone:
rotates flat-pack instructions into a physical object
turns a map to match the direction they are facing
visualises how a parked car must angle into a space
Paper folding and unfolding
These items present a folded shape, sometimes with holes punched into it, and ask what the pattern would look like once unfolded.
This type of task is useful because it taps sequential visualisation. The person must hold several transformations in mind at once.
A student may struggle here even if they perform well on simple shape matching. That tells you the issue may be complexity of transformation rather than basic perception.
Tip: If a learner says, “I can see the first fold but then I lose it,” that comment is clinically useful. It suggests a breakdown during multi-step manipulation, not necessarily a lack of understanding.
Block counting
Block counting tasks show a stack of cubes and ask how many total blocks are present, including hidden ones.
These items often reveal whether a person can infer structure from incomplete visual information. This matters in STEM learning, but also in practical tasks like building, stacking, or estimating unseen supports.
A child who counts only the visible blocks may not be careless. They may find it hard to infer what is concealed in three-dimensional space.
Object assembly
Object assembly presents separate parts and asks what whole object they would form.
This format has particular relevance beyond occupational testing. In military selection research, the Assembling Objects measure showed small but meaningful added value beyond the standard ASVAB, with incremental validity of 0.013 for training school grades and 0.03 for hands-on performance tests among U.S. Army recruits in a battery that included spatial measures (National Academies chapter 8)).
That same line of evidence is notable for fairness. In Project A analysis, the male-female effect size for Assembling Objects was relatively small, lower than several other spatial tasks in the same body of work, which is one reason many professionals view object assembly as a promising format when equity matters.
Adaptive digital formats
Paper tasks still have value, but many settings now use digital versions. One example from workforce testing is the SHL Verify Spatial Ability Test, an adaptive assessment with an average testing time of 15 minutes and up to 22 questions. It can reduce administration time by up to 30% compared with fixed-form tests, and the linked fact sheet reports a correlation of r = 0.72 with on-the-job success in manufacturing and aviation, with top-quartile scorers showing 25% faster task completion in simulations (SHL Verify Spatial Ability Test fact sheet).
That matters in clinical and educational thinking too. Adaptive systems can shorten fatigue-heavy sessions while still sampling a wide range of difficulty.
For professionals thinking about how visual-spatial demands interact with motor output, the relationship to visual-motor integration Beery is often worth keeping in mind.
A quick comparison
Test format | What it asks | What it often reveals |
|---|---|---|
Mental rotation | “Which shape is the same object turned?” | Internal manipulation of form |
Paper folding | “What happens after folds and openings?” | Multi-step visual transformation |
Block counting | “How many cubes are really there?” | Hidden structure and 3D inference |
Object assembly | “Which whole comes from these parts?” | Part-to-whole integration |
When you choose a spatial abilities test, the item format is not cosmetic. It determines what kind of thinking you are measuring.
Making Sense of the Scores
A score only becomes useful when it changes what you do next. That is where many people get stuck. They receive a percentile, a standard score, or a profile chart and ask, “So what does this mean for this child, this student, or this patient?”
The answer depends on whether you are reading the result normatively or clinically.
Normative reading
A normative interpretation compares one person to a reference group. It helps answer whether performance is lower, average, or higher than expected for age or educational stage.
That matters when identifying unusual strengths and unusual needs. A strong object assembly score may point to overlooked engineering or design potential. A weak rotation score may help explain why a capable learner struggles with geometry diagrams or molecular models.
Normative comparison is useful, but it should never be the whole story.
Clinical reading
Clinical interpretation asks a different question. It looks at the pattern.
For example:
low spatial performance with strong verbal reasoning may suggest a highly uneven profile
weak visual-spatial scores plus poor constructional output may affect handwriting, maths layout, or dressing
reduced spatial orientation after neurological injury may shape mobility and safety planning
The profile often matters more than a single total score.
Sub-skills matter
One reason subtests help is that spatial ability is not a single lumped trait in practice. The Johns Hopkins Center for Talented Youth Spatial Test Battery separates skills such as Surface Development and Block Rotation. In Canadian cohorts, STB scores predicted 35% of the variance in STEM course performance, and students with lower scores, defined as below the 40th percentile, showed an 18% improvement after a 12-week visualisation training programme (understanding STB scores).
That kind of evidence matters because it reframes scores as a starting point for intervention rather than a fixed label.
Key point: A low spatial score should prompt questions, not conclusions. Ask what task demands broke down, under what conditions, and what support changed performance.
What to look for when interpreting results
A careful reading usually includes these checks:
Age fit A task may be valid in one age group and less informative in another.
Demand overlap Some tasks mix spatial reasoning with speed, motor precision, or attention.
Context A student who struggles in geometry may need a different interpretation from an adult in stroke rehabilitation.
Convergence Do classroom observations, therapy findings, and test scores tell a similar story?
Stability If scores will shape major decisions, reliability matters. For professionals reviewing repeat measurement, this guide on reliability test-retest is a useful reference point.
A practical lens
Consider two learners.
One scores lower on block rotation but performs adequately on verbal explanations. That learner may benefit from concrete models, drawing steps, and slower visual transformation demands.
Another shows high part-to-whole assembly skill despite average reading performance. That student may be ready for design, robotics, engineering enrichment, or project-based learning that traditional academic screening overlooked.
The score is not the story. The interpretation is what turns a number into support.
Spatial Skills in Clinical and Educational Practice
Spatial testing remains underused where it could do the most good.
In schools, many gifted and support systems still lean heavily on verbal and mathematical measures. In clinics, many cognitive screens favor language, recall, and broad orientation questions while giving limited attention to richer spatial processing.
That creates blind spots.
In education
California provides a striking example. Spatial abilities tests are described as severely underrepresented in gifted education, even though gifted programmes serve over 100,000 students annually. The same report notes that only 8% of identified gifted students come from the lowest socioeconomic quartile, and suggests that including spatial tests could raise that figure by 15% to 20% (ERIC report ED660319).
This is not a small administrative issue. It shapes who gets seen as talented.
A child who does not stand out on reading-heavy measures may still have exceptional potential in design, engineering, architecture, technical drawing, robotics, or hands-on problem solving. If schools never measure those abilities, they systematically miss students whose strengths are non-verbal and visual.
In rehabilitation and clinical care
Spatial assessment also changes care planning.
A therapist working with dyspraxia, stroke, brain injury, or developmental coordination concerns often needs more than a general statement such as “cognition mildly affected.” Daily functioning depends on whether the person can judge distance, organise movement in space, understand part-whole relations, and maintain orientation during action.
That can influence:
Home safety planning
Route training
Dressing strategies
Handwriting or classroom accommodation
Choice of therapy activities
Referral decisions for broader neuropsychological assessment
Why broad screening misses the problem
Many standard tools tell you whether someone remembers words or follows instructions. They may not tell you why a child cannot align digits in long division or why an older adult reaches inaccurately for a cup on the table.
Spatial assessment fills that gap by making the invisible visible.
Consider these examples:
Setting | What people notice first | What spatial testing may clarify |
|---|---|---|
Classroom | Poor geometry confidence | Difficulty with visualisation or rotation |
Paediatrics | Puzzle avoidance, messy spacing | Weak spatial relations or planning |
Rehab | Trouble navigating familiar rooms | Orientation or perception deficit |
Counselling or psychology | “Smart but uneven” profile | Verbal-spatial discrepancy |
A better use of the test
The most helpful way to use a spatial abilities test is not as a gatekeeper but as a targeting tool.
In education, it can support enrichment, accommodation, or referral for further evaluation.
In clinic work, it can guide what to observe in functional tasks. If a patient struggles on orientation-heavy tasks, therapy may need more body-in-space work. If assembly and construction are the weak points, intervention may focus on sequencing, modelling, and graded visual-motor tasks.
Practical advice: If a concern appears in daily life, test the practical application of that skill. Do not rely on a broad global score alone.
Spatial skill affects outcomes that matter to families and professionals. It affects confidence, independence, access to STEM pathways, and the precision of rehabilitation planning. That is why this area deserves more attention than it usually gets.
The Digital Revolution in Cognitive Assessment
Traditional spatial testing often creates a familiar problem. The tasks may be useful, but the process can be slow, static, and detached from intervention. Paper forms also make it harder to capture how a person approached the task, where they slowed down, or what happened across repeated trials.
Digital assessment changes that.

Why digital tools fit spatial tasks well
Spatial reasoning is visual by nature. Screens can present rotation, transformation, motion, and pattern changes more naturally than static paper in many cases.
They also allow:
Adaptive difficulty so easy and hard items can be matched to the user
Shorter sessions that reduce fatigue
Game-like presentation that may feel less threatening for children
Repeated measurement for tracking progress over time
These are not cosmetic changes. They affect access and usefulness.
The clinical need is real
In California healthcare, providers are described as lacking validated spatial tests for clinical screening, even though spatial impairments affect 40% of neurodiverse cases according to the verified data set tied to the cited review source. The same verified data notes that recent Southern California rehabilitation trials of OrangeCheck showed 25% faster profiling in under 30 minutes, with 92% clinician satisfaction (PMC review context and linked verified summary).
Those figures matter because they point to a practical issue. Professionals need assessment that fits into real workflows.
One option in this newer ecosystem is Orange Neurosciences, which offers digital cognitive assessment and training tools designed to profile domains including perception and visual-spatial skills in a brief format. For readers looking at remote or hybrid workflows, their overview of cognitive assessment online shows how this category of platform is being framed for practice use.
Assessment and intervention should talk to each other
The older model often looks like this: test once, write a report, make general recommendations, and hope the intervention matches the profile.
Digital platforms can tighten that loop.
A stronger workflow is:
Measure the spatial profile
Identify the specific weak point
Assign targeted practice or therapy
Reassess using comparable tasks
Adjust the plan based on response
That model is especially valuable when the concern is changing over time, such as school intervention, concussion recovery, rehabilitation, or neurodevelopmental monitoring.
Professional benefit: The most useful digital systems do not only tell you whether someone got an item right. They help you see patterns that can shape what you do next.
Better access, if used carefully
Digital tools are not automatically better. They still need good psychometrics, age-appropriate design, and ethical use. They also should not replace clinical judgment.
But when used well, they reduce friction. They make spatial assessment easier to repeat, easier to scale, and easier to connect to action. For a field where spatial ability has long been measured less often than it should be, that shift is important.
Putting Knowledge Into Action Your Next Steps
If spatial concerns are on your radar, the next step is not to hunt for a single magic score. The next step is to match the question to the right kind of assessment.
A teacher may ask why a student who speaks well struggles in geometry. A developmental paediatrician may ask whether puzzle avoidance reflects motor difficulty, spatial reasoning weakness, or both. A rehabilitation team may ask whether navigation errors are improving over time. Each question calls for a slightly different use of a spatial abilities test.
For educators
Start with the classroom concern.
If the issue is diagram-heavy maths, construction, or STEM participation, look for tools that separate visualisation from broader academic attainment. If the concern is hidden strength, consider whether current identification methods rely too heavily on verbal and maths scores alone.
Useful next moves include:
Reviewing referral criteria so spatial skill is not excluded by default
Collecting work samples such as model building, geometry reasoning, or design tasks
Using spatial findings to guide support, not only selection
Tracking response to intervention rather than treating one result as fixed
For clinicians and therapists
Focus on function.
Ask which daily tasks break down. Is the person getting lost, misjudging reach, struggling with assembly, or finding visual-motor tasks unusually effortful? Then choose assessment formats that mirror those demands as closely as possible.
A practical process often looks like this:
Step | Question to ask |
|---|---|
Identify the complaint | What is hard in daily life or learning? |
Map the skill | Is this visualisation, orientation, relations, or visual-motor overlap? |
Select the tool | Which task format samples that skill best? |
Interpret in context | Does the score fit the observed pattern? |
Act on it | What changes in teaching, therapy, or referral follow from this? |
For parents and individuals
If you are seeking answers, bring examples rather than labels.
Instead of saying “I think my child has bad spatial skills,” say what you see:
they reverse directions under pressure
they avoid construction toys
they understand lessons verbally but struggle with diagrams
they bump into furniture or misjudge space
they take much longer on assembly or copying tasks
That kind of detail helps professionals decide whether a spatial abilities test belongs in the assessment plan.
What to look for in a modern option
Whether you are comparing clinic-based tools, school-based screening, or digital platforms, ask practical questions:
Does the test separate sub-skills or give only one broad score?
Is it appropriate for the person’s age and setting?
Can results guide intervention, accommodation, or referral?
Can progress be reassessed without unnecessary burden?
Does the format reduce stress enough for the person to show their ability?
The best next step is usually not more guessing. It is better observation, better measurement, and a clearer bridge from results to action.
If you want a practical way to explore digital cognitive profiling and intervention pathways, visit Orange Neurosciences or contact their team by email to see how spatial and related cognitive skills can be assessed and tracked within everyday clinical or educational workflows.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation