Personality Assessment Inventory A Clinical Guide
May 13, 2026

You're often handed the same kind of referral. The person reports poor concentration, mental fatigue, irritability, low mood, and trouble functioning at work or at home. A brief interview suggests anxiety. A cognitive screen hints at slowed processing or reduced working memory. A family member says, “This has always been part of their personality.” The chart already contains two previous labels that don't fully fit.
That's where the personality assessment inventory can help. Not because it gives a magical answer, but because it imposes structure on a messy presentation. Used well, it helps you sort enduring personality style from acute distress, identify response patterns worth questioning, and turn scattered complaints into a more coherent formulation.
Untangling Complex Cases with Deeper Assessment
A common clinical puzzle looks simple at first. A patient says they can't focus, forgets appointments, feels overwhelmed, and has become socially withdrawn. If you only hear “poor focus,” you might lean toward ADHD, concussion effects, burnout, depression, or all of them at once.
That's usually where confusion starts. Cognitive complaints don't tell you whether the primary driver is mood, stress, personality organisation, coping style, or a true decline in cognitive efficiency. They only tell you the person is struggling.
When symptoms overlap
Consider an adult outpatient who reports lifelong distractibility but also recent panic, unstable relationships, and frequent feelings of emptiness. If you rely only on symptom checklists, it's easy to mistake a broad pattern of dysregulation for a narrow attentional disorder. If you rely only on interview impressions, you may overread dramatic presentation and miss the patient's actual profile.
The personality assessment inventory helps because it asks a different question. Not just “What symptoms are present?” but “How is this person describing themselves across multiple domains, and does that pattern hang together?”
A useful way to explain this to patients is to compare it to looking at a map rather than a single street. A complaint like “I can't concentrate” is one street. A full personality profile shows whether that street runs through anxiety, depression, interpersonal distrust, treatment resistance, or a broader behavioural pattern.
For adults with overlapping attentional, autistic, and mood-related concerns, a more individualized pathway can also be helpful. Colleagues and patients looking for specialized assessment for AuDHD adults may find that kind of focused diagnostic work useful when the usual categories don't capture the whole picture.
Why deeper assessment matters in practice
The PAI's value isn't academic. It's practical. It can sharpen questions like these:
Is this distress broad or circumscribed? A patient may present with memory complaints, but the wider profile may point more strongly to anxiety, stress, and somatic focus.
Is the self-report interpretable? Before you trust any profile, you need to know whether the response style appears reasonably consistent and credible.
What could derail treatment? Some patients aren't just symptomatic. They're ambivalent, mistrustful, unsupported, or unlikely to engage.
Clinical reality: The hardest cases are rarely “unclear” because no symptoms are present. They're unclear because too many plausible explanations fit at once.
If you want a broader orientation to how personality testing sits beside cognitive and neuropsychological work, this guide to what neuropsychological assessment involves gives a useful clinical frame.
Understanding the Personality Assessment Inventory
A common referral looks straightforward on paper. An adult reports poor concentration, rising irritability, and inconsistent follow-through. Brief cognitive testing may show slowed efficiency or weak working memory, but that still leaves an open question. Are we looking at primary attention problems, depression, chronic stress, a defensive response style, or several of these at once? The Personality Assessment Inventory, or PAI, was built for that kind of clinical ambiguity.
The PAI is a structured self-report measure of adult personality and psychopathology developed by Leslie C. Morey. It was first published in 1991 and revised in 2007. In practice, its value comes from how it organizes a patient's own report into patterns a clinician can test against interview findings, behavioural observations, and cognitive data.
The mechanics are straightforward. The PAI includes 344 items, uses a 4-point response scale, and usually takes less than an hour to complete. Patients rate statements from 0 = False, not at all true to 3 = Very true. That simple format matters. A test can be clinically rich without being difficult to administer, score, or explain, which is one reason the PAI fits well into outpatient practice, rehabilitation settings, and diagnostic workups where time is limited.
What makes the measure clinically useful is its breadth without becoming chaotic. The PAI includes 22 non-overlapping scales that cover validity, clinical symptoms, treatment-related factors, and interpersonal style. That design helps the clinician answer several different questions at the same time. Is the person describing distress in a reasonably consistent way? Which symptom clusters stand out? What might complicate treatment engagement? How does the person typically relate to other people?
A simple way to explain this to patients is to compare it to hearing an orchestra one section at a time. Cognitive testing may tell you how well the instrument is functioning. The PAI helps you hear the emotional, behavioural, and relational patterns playing around it. When both are interpreted together, the clinical picture is usually sharper than either source alone.
That integrated view is part of the modern standard of care. A patient with memory complaints, for example, may show average learning on cognitive measures but increased anxiety, somatic concern, and stress on personality assessment. Another patient may perform unevenly on attention tasks while also showing a response style that calls for caution before drawing firm conclusions. In cases like these, the PAI does not replace cognitive assessment. It adds context that helps the clinician decide what the scores mean in real life, and whether the pattern is likely to hold up over time. That is one reason familiarity with test-retest reliability in psychological assessment helps when interpreting PAI findings alongside neuropsychological data.
Clinicians keep using the PAI because it supports formulation, not just description. It helps convert a long symptom list into practical questions about risk, engagement, coping style, and differential diagnosis. Research and test publisher materials also describe it as a psychometrically established tool with wide clinical use in adult assessment settings (NZCER PAI overview).
A good personality inventory gives formulation better raw material.
Navigating the PAI Scale Structure
The PAI becomes much easier to use when you stop seeing it as a list of abbreviations and start seeing it as a set of clinical questions. Each cluster answers a different question about the patient.
Four functional clusters
Scale Cluster | Purpose | Example Scales |
|---|---|---|
Validity | Checks whether the response pattern is interpretable | Inconsistency, Infrequency, Negative Impression Management, Positive Impression Management |
Clinical | Profiles emotional, behavioural, and psychiatric symptoms | Somatic Complaints, Anxiety, Depression, Paranoia, Borderline Features, Antisocial Features |
Treatment | Highlights factors that affect care planning and risk | Aggression, Suicidal Ideation, Stress, Nonsupport, Treatment Rejection |
Interpersonal | Maps habitual style with other people | Dominance, Warmth |
Validity scales as quality control
Start here every time. If the validity picture doesn't make sense, the rest of the profile may not deserve much weight.
A simple analogy helps. Think of validity scales as the calibration check on a blood pressure cuff. You can still get a number when the device is off, but that number may lead you in the wrong direction.
In practice, these scales alert you to things like inconsistent responding, unusual endorsement patterns, or highly defensive or highly negative self-presentation. They don't prove deception. They tell you to slow down.
Clinical scales as symptom profilers
These are the scales most clinicians look for first, but they shouldn't be interpreted in isolation. A high depression score means something different in a profile marked by severe stress and suicidal ideation than in a profile marked by chronic interpersonal instability and suspiciousness.
That's why I encourage colleagues to read the profile as a shape, not a set of isolated peaks. The question isn't “Is depression high?” The question is “What rises with it, and what stays flat?”
A few examples:
Somatic Complaints can help clarify whether bodily symptoms are central to the patient's distress narrative.
Anxiety may point toward pervasive tension, worry, and arousal.
Borderline Features can signal affective instability, identity disturbance, and volatile relationships.
Antisocial Features may be relevant when rule-breaking, impulse control, and externalisation are in the foreground.
Treatment scales as early planning tools
These scales are often underused. That's a mistake, because they often tell you what will happen after the assessment report is filed.
If a patient shows marked stress, low support, and resistance to treatment, you don't just have a symptom profile. You have a workflow problem. They may miss appointments, disengage early, or reject interpretations that feel threatening.
Practical rule: Read the treatment scales as barriers to implementation. A brilliant treatment plan that the patient won't enter is still a poor plan.
The Treatment Rejection scale is a good example. It can act like an early warning light. If high, it may tell you the person doesn't see themselves as needing help, doesn't trust intervention, or doesn't want to be psychologically understood.
For clinicians who want a refresher on how to think about score stability over time, this overview of test-retest reliability is worth revisiting.
Interpersonal scales as relationship maps
These scales often explain why treatment feels easy with one patient and unexpectedly strained with another. They offer a sketch of the person's usual stance with other people.
A highly dominant profile may push back hard against guidance. A low warmth profile may seem detached or difficult to engage. Neither finding is “bad.” Both matter clinically.
That matters in feedback sessions. If a patient is likely to experience questions as intrusive or corrective comments as critical, you can adjust your style before the alliance starts to fray.
From Raw Scores to Actionable Clinical Insights
A report lands on your desk after a patient complains of forgetfulness, low motivation, and slipping work performance following a medical event. The referral question sounds cognitive. The PAI helps you decide whether the problem is primarily depression-related inefficiency, stress-related overload, emerging personality complications, or some combination that changes what you do next.
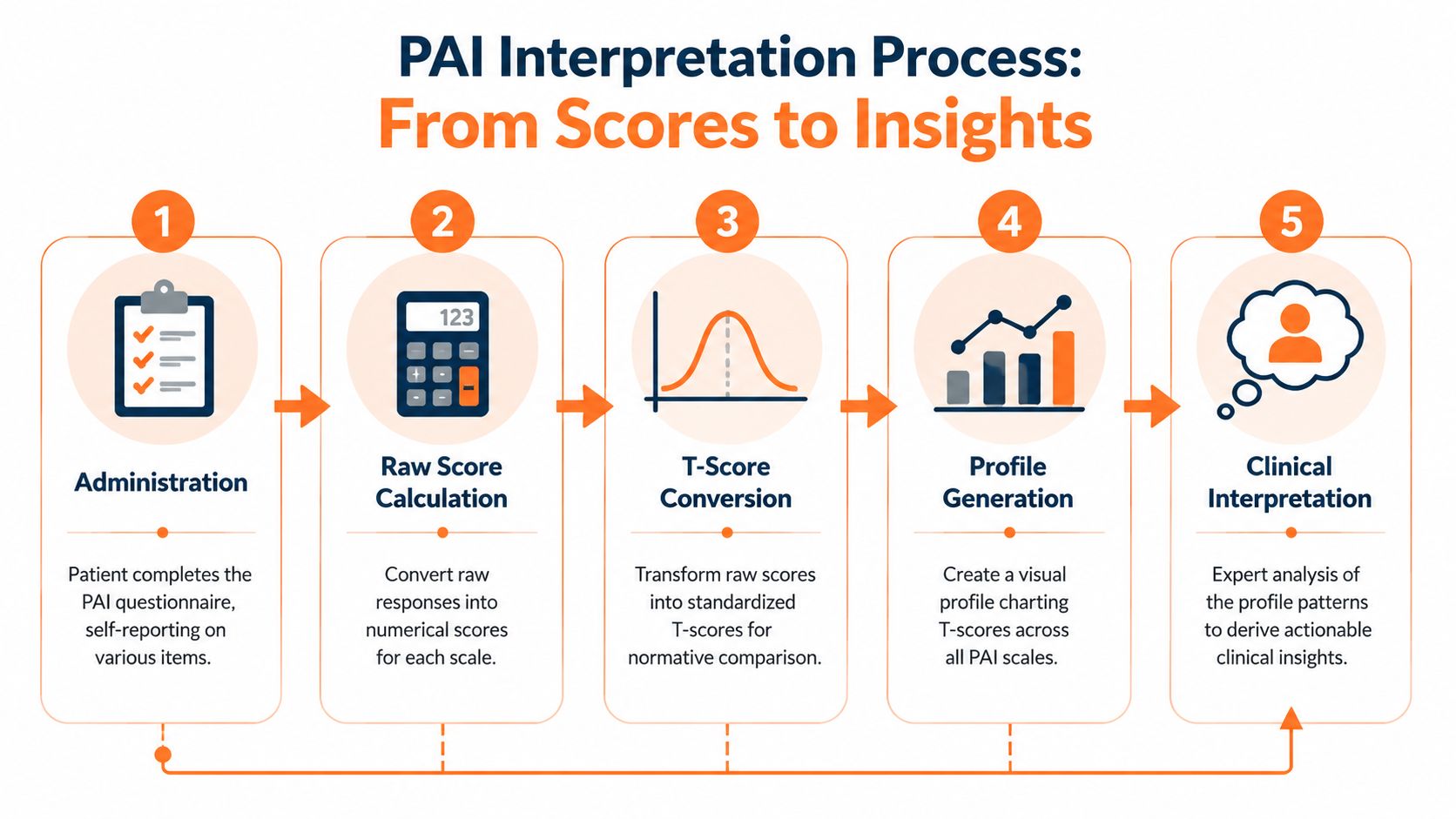
Start with the reference frame
PAI interpretation works a lot like reading a blood pressure value. The number has meaning only in relation to the right reference group, the right context, and the right question. In Canadian high-stakes work, analysts reviewing Canadian high-stakes PAI use found that outdated community norms can push T-scores upward enough to create false clinical flags.
That is not a technical footnote. It changes case formulation. A profile can appear more pathological than it is if the comparison group is wrong.
So the first clinical question is simple. Which norms fit this patient and this setting?
A practical reading sequence
Trainees often want to jump to the highest score. That is understandable, but it usually produces shallow interpretations. A better method is to read the profile in the same order you would assess a patient in person.
Establish interpretability
Review validity scales first. If inconsistency, exaggeration, or defensiveness is prominent, the profile may still be useful, but only with clear limits.Identify the main pattern
Look for clusters, not isolated peaks. Depression plus anxiety plus stress burden suggests a different clinical picture than depression plus paranoia or depression plus aggression.Translate scales into mechanisms
Ask what may be driving day-to-day impairment. Is the patient slowed by hopeless thinking, flooded by tension, distracted by trauma-related arousal, or derailed by interpersonal conflict?Connect findings to treatment decisions
The same symptom severity can call for different care plans. A patient with marked distress and intact help-seeking may tolerate direct intervention. A patient with distress plus mistrust may need a slower alliance-building approach.Compare with cognitive data The PAI becomes especially useful in modern practice for this purpose. Self-reported cognitive difficulty may reflect depression, anxiety, pain, fatigue, poor effort, neurologic change, or several at once. The profile helps you sort those possibilities before you over-attribute every complaint to brain dysfunction.
Example of clinical translation
Consider a patient whose history includes a recent concussion, persistent forgetfulness, and trouble finishing routine tasks. The validity scales are acceptable. Clinical scales show depressive thinking and high stress, while treatment scales suggest the person feels alone but remains open to help.
That pattern should change how you interpret the referral question. Instead of concluding that the patient has a straightforward cognitive decline, you would hold a more precise hypothesis: mood and stress may be reducing efficiency, especially for planning, initiation, and sustained attention. In practice, that means cognitive testing remains useful, but the interpretation must account for emotional load.
The Depression-Cognitive subscale is often helpful here. As noted earlier, higher scores on that subscale have been associated with executive dysfunction in relation to neurocognitive batteries. That does not prove neurological impairment. It tells you the complaint deserves direct follow-up, ideally with cognitive data that can separate subjective burden from measurable deficit.
This is the bridge between academic theory and clinical reality. A PAI score earns its place when it changes what happens next, such as whether you refer for fuller neuropsychological testing, start mood treatment first, adjust expectations for rehabilitation, or explain the symptoms in a way the patient can accept. For a broader comprehensive diagnostic overview, it helps to place personality and symptom data alongside cognitive measures rather than treating them as separate tracks.
Common interpretation errors
Several mistakes show up again and again in reports.
Overreading one scale. A single elevation is a clue, not a conclusion.
Ignoring subscales. Broad scales tell you where the distress sits. Subscales often tell you how it operates.
Skipping the functional question. Every interpretation should answer, “How will this affect treatment, adherence, safety, or cognitive performance?”
Writing labels instead of formulations. “High depression” is less useful than “depressive pessimism and low energy are likely reducing initiation and mental efficiency.”
Separating personality findings from cognitive findings. In integrated care, those data streams should inform each other.
A good cross-check is to use the same discipline you would use when interpreting Beck Depression Inventory scores in practice. The number starts the conversation. Clinical judgment, context, and corroborating evidence determine what the number means.
Strong PAI interpretation explains how the patient functions, why the pattern appears, and what the clinician should do differently because of it.
Key Clinical and Research Applications of the PAI
A referral looks straightforward until the interview starts. The patient reports poor concentration, missed appointments, conflict at home, and rising frustration with treatment. On paper, that can resemble depression, a stress response, poor insight, personality pathology, or a cognitive problem. In practice, the PAI helps sort those possibilities into a more usable clinical picture.

The PAI's value is not that it produces labels. It helps clinicians answer applied questions. What is getting in the way of care? Which risks need closer monitoring? Which apparent cognitive complaints may be amplified by distress, distrust, or low treatment engagement? That practical focus is why the instrument remains useful across clinical, forensic, rehabilitation, and research settings.
Forensic and custody work
Forensic referrals usually ask narrower questions than ordinary outpatient care. A court may want to know how a parent handles stress, whether anger is controlled or poorly regulated, or whether suspiciousness and interpersonal instability are likely to affect judgement. The PAI can contribute to that formulation because it samples response style, affective distress, aggression-related tendencies, and interpersonal patterns in one structured format.
When used correctly, this tool functions as a pressure test. It does not determine custody, competence, or risk independently. Instead, it assists the evaluator in examining how an individual is likely to function when demands increase and relationships become strained. In custody evaluations, for instance, increased aggression, paranoia, or borderline features may matter less as isolated findings than as part of a pattern suggesting inconsistent parenting, conflict escalation, or difficulty tolerating the needs of the child.
That is also where restraint matters most. High-stakes settings punish overstatement. A careful clinician treats the PAI as one strand of evidence alongside records, behavioural observations, collateral interviews, and the specific legal question.
Rehabilitation and treatment planning
Rehabilitation teams often face a familiar puzzle. The treatment plan is reasonable, the goals are clear, and the patient still misses sessions, disengages, or rejects recommendations. In those cases, the PAI can clarify whether the obstacle is mood disturbance, somatic focus, mistrust, anger, low motivation for treatment, or a longstanding interpersonal style that makes alliance difficult.
This changes care in concrete ways.
A patient with marked treatment rejection and suspiciousness may need slower rapport-building, more transparent explanations, and shared goal-setting before intensive therapy begins. A patient with strong anxiety and somatic preoccupation may benefit from repeated reassurance, simple behavioural targets, and coordination between medical and mental health staff so the message stays consistent. The score pattern guides the first moves, much like a map helps you choose the safest route before the drive starts.
Research use and convergent validity
In research, the PAI is useful because it translates complicated clinical phenomena into dimensions that can be studied across settings. Investigators use it to examine symptom patterns, treatment response, response distortion, and overlap between personality features and psychiatric presentations. That makes it valuable in studies that need more nuance than a single diagnosis can provide.
Its research role also supports everyday clinical confidence. When a measure shows meaningful convergence with other established personality instruments, clinicians can interpret findings with more assurance that they are tracking recognizable constructs rather than test-specific noise. The instrument is still not interchangeable with every other tool. It holds a credible place in a larger assessment framework.
Medical and neuropsychological settings
Medical and neuropsychological referrals often involve the hardest kind of differential question because emotional and cognitive symptoms can mimic each other. A patient may report memory failure, slowed thinking, irritability, and fatigue. The clinician then has to ask whether those complaints primarily reflect neurological change, emotional distress, maladaptive coping, or some mixture of all three.
The PAI helps sharpen that distinction by adding information about mood, anxiety, somatic concern, defensiveness, and treatment attitude. That is particularly helpful when paired with cognitive assessment tools used in neuropsychological practice, because the two data streams answer different clinical questions. One captures self-reported emotional and interpersonal functioning. The other shows how the person performs on tasks that require attention, memory, speed, or executive control.
That combined view is where theory becomes better care. A profile marked by severe anxiety and rumination may explain why a patient performs below expectation on demanding cognitive tasks. A profile marked by minimisation or low insight may explain a mismatch between reassuring self-report and obvious functional decline. Integrated interpretation gives the team something more useful than a score summary. It gives a plan.
For readers who want a wider view of where mental health assessment is heading, this comprehensive diagnostic overview offers useful context.
Integrating PAI with Cognitive Assessments
No personality tool should stand alone. The best use of the PAI happens when it is paired with data about how the person thinks, processes, remembers, and sustains effort.

Personality data and cognitive data answer different questions
A simple distinction helps.
The PAI tells you how the person reports distress, coping, relationships, and treatment-relevant features.
A cognitive assessment tells you how the person performs on tasks involving attention, memory, executive function, speed, or related abilities.
Both are necessary because patients often blur them together. Someone may say, “My memory is terrible,” when the primary problem is severe anxiety and intrusive rumination. Another may minimise distress while objective testing shows meaningful cognitive inefficiency.
That's why integrated assessment is so useful. One tool captures the lived psychological experience. The other checks functional cognitive performance.
How this compares with the MMPI in practice
Clinicians often compare the PAI with the MMPI family. In day-to-day work, the difference is less about which one is “better” and more about fit.
The PAI is often experienced as more direct and easier to map onto practical treatment questions. Its structure is relatively accessible to explain to patients and trainees. The MMPI has its own strengths, particularly in settings where its extensive interpretive traditions matter, but many clinicians find the PAI easier to use when the goal is a focused, clinically digestible profile rather than a denser personality assessment ecosystem.
The key point is this. Whether you choose the PAI or another personality measure, you still need objective cognitive data when the referral includes memory, processing, attention, or executive concerns.
The evidence gap matters
There's an important limitation here. While the PAI is well researched in psychopathology, there is minimal peer-reviewed content on its utility in neurodevelopmental assessment or cognitive rehabilitation, including examples such as ADHD and stroke recovery, according to the POST publication discussing these gaps.
That gap has practical consequences. Clinicians still lack clear guidance on how personality constructs measured by the PAI predict success in cognitive training, or how best to integrate personality findings with rapid objective cognitive metrics. In other words, the field knows these domains should talk to each other. It has not fully shown us the best script yet.
We can already see the clinical need even where the literature is still catching up.
A workable integrated model
In real practice, an integrated approach often looks like this:
Use the PAI when emotional distress, personality style, or treatment engagement may be shaping the case.
Use objective cognitive tools when the patient reports problems with memory, speed, attention, or executive control.
Interpret both together rather than letting one dominate.
For example, a patient in rehabilitation may show high self-reported stress and depressive cognition on the PAI, while objective testing shows slowed processing but relatively preserved memory. That combined picture supports a different intervention plan than either measure alone.
If you're comparing options for the cognitive side of that workflow, this review of cognitive assessment tools is a practical starting point.
Ethical Considerations for Your Clinical Workflow
The personality assessment inventory is useful. It can also be misused. Most of the ethical problems arise not from the instrument itself, but from how confidently people interpret it without enough context.
Best practices worth keeping in routine use
A responsible workflow usually includes the following:
Use appropriate norms: If the normative reference is a poor fit for the patient or setting, your interpretation may overpathologise ordinary variation.
Treat validity scales as a prompt for caution, not accusation: An unusual response style is not the same thing as dishonesty.
Integrate multiple data sources: Interview, records, behavioural observations, collateral information, and cognitive findings all matter.
Explain findings in ordinary language: Patients should leave feedback understanding patterns, not feeling branded by jargon.
Tie results to decisions: Every major interpretation should influence treatment planning, monitoring, or referral choices.
Multicultural and contextual care
This point deserves emphasis. Personality measures are especially vulnerable to misinterpretation when clinicians assume that all patients read, respond, disclose, and understand distress in the same way.
Cultural background, language, education, familiarity with testing, and prior experiences with institutions all shape self-report. A guarded profile may reflect mistrust, fear of consequences, or misunderstanding. A highly distressed profile may reflect lived adversity as much as psychopathology.
That means ethical use of the PAI requires humility. Not less interpretation, but more careful interpretation.
A defensible report names its limits. It doesn't hide them.
Giving feedback without doing harm
Feedback sessions are where technical competence becomes human competence. The patient usually doesn't care that a scale is high. They care what it means for their life.
That translation can be gentle and still precise. Instead of saying, “You have prominent borderline features,” you might say, “Your responses suggest strong emotional swings, sensitivity in relationships, and periods of feeling unsure of yourself. That helps explain why stress can feel so hard to contain.”
That kind of language preserves dignity while keeping clinical meaning. It also makes treatment recommendations more likely to be accepted.
For clinicians who want to improve how they communicate findings, this guide on the language of assessment is worth keeping close at hand.
The main takeaway
Use the PAI as part of a thoughtful assessment system, not as a shortcut. Its best role is to deepen formulation, sharpen treatment planning, and complement other forms of evidence, especially when personality, distress, and cognition are all in play.
When you work that way, the personality assessment inventory becomes what it should be. Not a label-maker, but a clinical tool that helps people get more accurate care.
Orange Neurosciences helps clinicians bring that integrated model into everyday care. If you want objective cognitive profiling that complements personality assessment and supports faster, more precise decision-making, visit Orange Neurosciences or contact the team to explore how tools like OrangeCheck and ReadON can fit your workflow.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation