What Is Perception: Understanding Sensory Input

You're probably here because something felt off, but hard to name.
A child keeps losing their place when copying from the board. An older parent says “I can see it, but I can't make sense of it.” A patient hears a sound in a noisy room and turns the wrong way. Moments like these make people ask a very reasonable question. What is perception?
Many learn a simple answer: perception is what we see, hear, feel, smell, or taste. That's only part of the story. Our senses collect input, but the brain has to sort it, compare it with past experience, judge what matters, and build meaning from it. Perception is less like a camera recording the world and more like a skilled interpreter making fast decisions with incomplete information.
That's why two people can look at the same scene and notice different things. It's also why a bright, capable child can seem inattentive when the underlying difficulty is visual or spatial interpretation. If you work with behaviour, learning, rehabilitation, or ageing, perception often sits underneath the problems people describe first. It links closely with attention, memory, language, and movement, which is why a broader understanding of cognitive function is so useful in practice.
Perception isn't passive. The brain is constantly deciding what something is, where it is, and what to do about it.
When that process works smoothly, we barely notice it. When it falters, everyday life gets harder in subtle ways. Reading becomes tiring. Navigation feels effortful. Conversation in noisy settings breaks down. A person may even doubt their own abilities because the difficulty doesn't look obvious from the outside.
Introduction More Than What Meets the Eye
A common example happens in a crowd. You think you hear your name, turn around, and realise no one called you at all. Your ears picked up sound. Your brain filled in the rest.
That small “glitch” is a good doorway into understanding perception. Perception is the brain's active process of turning sensory input into a usable version of reality. It doesn't just receive information. It interprets it.
Why this matters in real life
For parents, this can explain why a child melts down in busy environments but seems fine in quiet, predictable spaces. For teachers, it can clarify why a student struggles with diagrams, spacing, or following multi-step movement tasks. For clinicians, it helps separate a sensory problem from a problem of interpretation, organisation, or response.
Here are a few practical examples:
In the classroom: A child may see every letter clearly but still confuse layout, spacing, or orientation on the page.
At home: An older adult may recognise a spoon in the drawer but hesitate when several similar objects are crowded together.
In rehabilitation: A patient may detect touch but misjudge where it occurred or how strong it was.
A better way to think about perception
If sensation is the brain receiving signals, perception is the brain asking: What is this? Does it matter? What does it mean?
That's why “what is perception” is more than a textbook definition. It's a practical question about how people function in ordinary life. It helps explain behaviour that might otherwise be labelled as careless, oppositional, anxious, or confused.
Clinical lens: When behaviour and ability don't seem to match, perception is often worth examining.
Perception can also be supported. Once you identify which part of the process is breaking down, you can choose better accommodations, better therapy goals, and better assessment tools. That shift matters. It moves us from guessing to observing, and from observing to measuring.
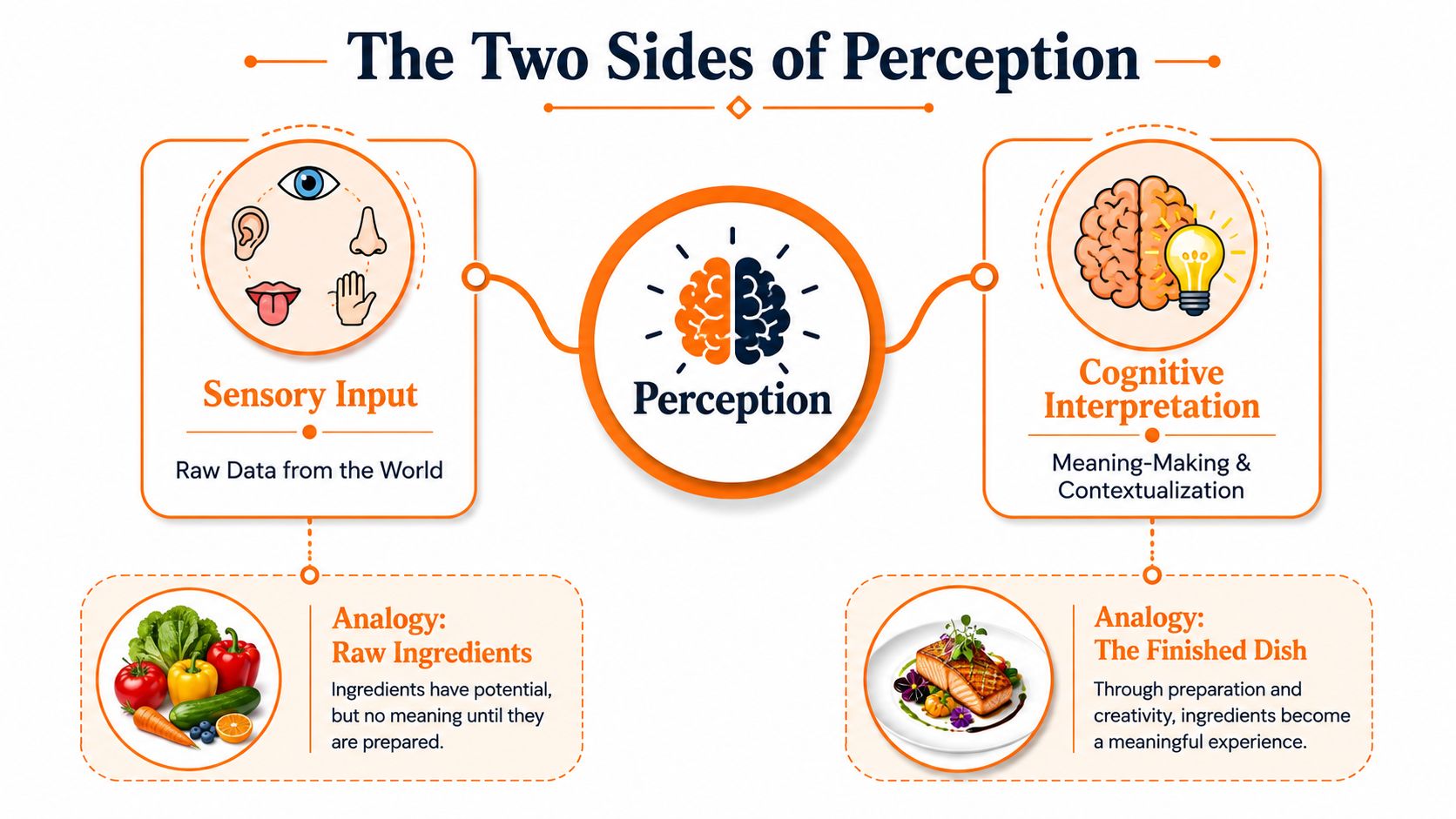
The Two Sides of Perception Sensory Input and Cognitive Interpretation
A useful way to separate the parts is to think like a cook.
Sensation is the raw ingredients. The vegetables, spices, oil, and grains are all there on the counter. Perception is the finished dish. The brain has selected, combined, and interpreted those ingredients into something meaningful.
Raw input is not enough
Your eyes detect light, edges, colour, and motion. Your ears detect vibration. Your skin detects pressure and temperature. None of that automatically becomes understanding.
The brain still has work to do:
Select what deserves attention.
Compare it with past experience.
Predict what is most likely.
Interpret the result in context.
That prediction step is where many readers get surprised. The brain doesn't wait for perfect information. It uses patterns from the world you've lived in before.
Why illusions work
Visual illusions aren't proof that perception is broken. They show how perception usually works. The brain makes educated guesses based on regular features of the environment, then sometimes those guesses misfire.
One overlooked example involves geometry. Research shows that angle and line perception is determined by statistical relationships between geometrical stimuli and their physical sources in typical environments, and data from the CA region shows that 32% of patients with neurodevelopmental disorders in paediatric clinics exhibit above-average difficulty in angular size discrimination, yet standard cognitive assessments rarely target this specific perceptual deficit (research on angular size discrimination and geometric perception).
That sounds technical, but the everyday meaning is simple. The brain learns from the shapes and layouts it sees repeatedly in the world. It doesn't just “see” an angle. It interprets that angle in light of what similar angles usually mean.
Why this gets missed
General explanations of perception often stop at the five senses. That leaves out spatial judgement, environmental prediction, and geometric interpretation.
This matters in practice because difficulties may show up as:
Trouble with maps or navigation: The person isn't merely distracted. They may be misreading spatial relationships.
Weak performance on copying tasks: The issue may involve angle judgement, not effort.
Problems with sports or movement planning: Fast interpretation of direction, distance, and shape may be the bottleneck.
A child who struggles with blocks, handwriting spacing, or judging corners in a room may not have a motivation problem. They may have a perception problem that's more specific than adults realise.
The Brain's Perception Engine Key Neural Pathways
Perception doesn't happen in one neat spot in the brain. It's a network job.
A significant part of the human cerebral cortex is devoted exclusively to visual processing, and neuroscientific findings show that brain network activity influencing conscious visual recognition originates in the ventromedial prefrontal cortex, or vmPFC, which influences both the sensitivity and criterion of conscious recognition (overview of visual perception and early brain processing).

The brain handles different questions at once
A simple way to understand this is through two broad visual jobs:
Brain job | Everyday question | Example |
|---|---|---|
Object identification | What is it? | Is that a cup or a candle? |
Spatial guidance | Where is it and how do I act? | How far away is it, and can I reach it safely? |
These pathways are often described as “what” and “where” streams. You don't need the formal terminology to see the clinical value. A person can struggle more with one than the other.
Someone may recognise an object but misjudge its location. Another person may see where something is but have trouble identifying it quickly. That distinction matters when choosing supports, therapy tasks, or further testing.
Higher-order regions shape what reaches awareness
Many people assume perception starts and ends in sensory cortex. In reality, higher-order regions help decide how incoming information is interpreted. The vmPFC is one example of that top-down influence.
That's part of why expectations, attention, and context can change what a person consciously recognises. It also helps explain why perception problems can appear subtle. The eyes may be healthy. Hearing may test as normal. Yet the person still struggles because the network responsible for meaningful interpretation is under strain.
For readers wanting a practical anatomy refresher, Orange's guide to the lobes of the brain gives a useful overview of how different regions contribute to real-world cognitive tasks.
The key takeaway is that perception is distributed. If you only look for one damaged sense organ or one obvious lesion, you can miss the problem.
When Perception Falters Clinical Examples of Impairment
Perceptual problems don't always look dramatic. Often they look confusing.
A person with visual agnosia may see an object clearly enough to describe its shape or colour, yet still fail to identify what it is. A person with prosopagnosia may recognise a voice immediately but not the face that goes with it. Another may walk carefully through a room, not because of weakness, but because depth and spacing feel unreliable.

What this looks like day to day
In children, perceptual difficulties may show up as poor puzzle skills, awkward spacing in writing, confusion with left and right, or distress in busy visual spaces. In adults, the signs can be more compensatory. They may avoid driving at night, rely heavily on labels and routines, or become anxious in crowded environments.
In older adults, the picture gets even more layered. Families may notice “confusion,” but the underlying issue might be visual interpretation, auditory filtering, or slowed integration of sensory cues. That's one reason broader context matters when reading about understanding Alzheimer's vs dementia. Not every perceptual problem means dementia, but perceptual change can be part of a larger cognitive story.
Perception thresholds can change with age
Perception also includes body-based detection, not only vision. In human somatosensory perception, the threshold for detecting contact current at intermediate frequencies from 300 kHz to 10 MHz is 20–30% higher than at 100 kHz, with older adults showing higher thresholds. This demonstrates that perception thresholds are frequency-dependent and age-dependent (study on contact current perception thresholds).
That finding matters because it reminds us that perception isn't fixed. The same physical input may not be experienced the same way across age groups.
A practical checklist for caregivers and clinicians
Missed recognition: The person sees or hears something but can't identify it reliably.
Spatial uncertainty: They bump into furniture, misjudge steps, or avoid unfamiliar layouts.
Sensory mismatch complaints: They say “it feels strange” even when basic sensory testing seems unremarkable.
Listening fatigue: In noise, they may seem inattentive when the problem is sorting and interpreting sound. If that's a concern, structured review of an auditory processing test can help frame the next step.
Perceptual impairment can be developmental, acquired, age-related, or part of another condition. What matters most is not to dismiss it as vague or behavioural before you've looked carefully.
How We Assess Perception From Observation to Objective Tests
Assessment usually starts informally. A parent notices clumsiness. A teacher sees difficulty copying shapes. A therapist hears repeated complaints about “not seeing it right” or “getting mixed up in space.”
Those observations matter. They often point us in the right direction. But observation alone rarely tells us which perceptual skill is weak.
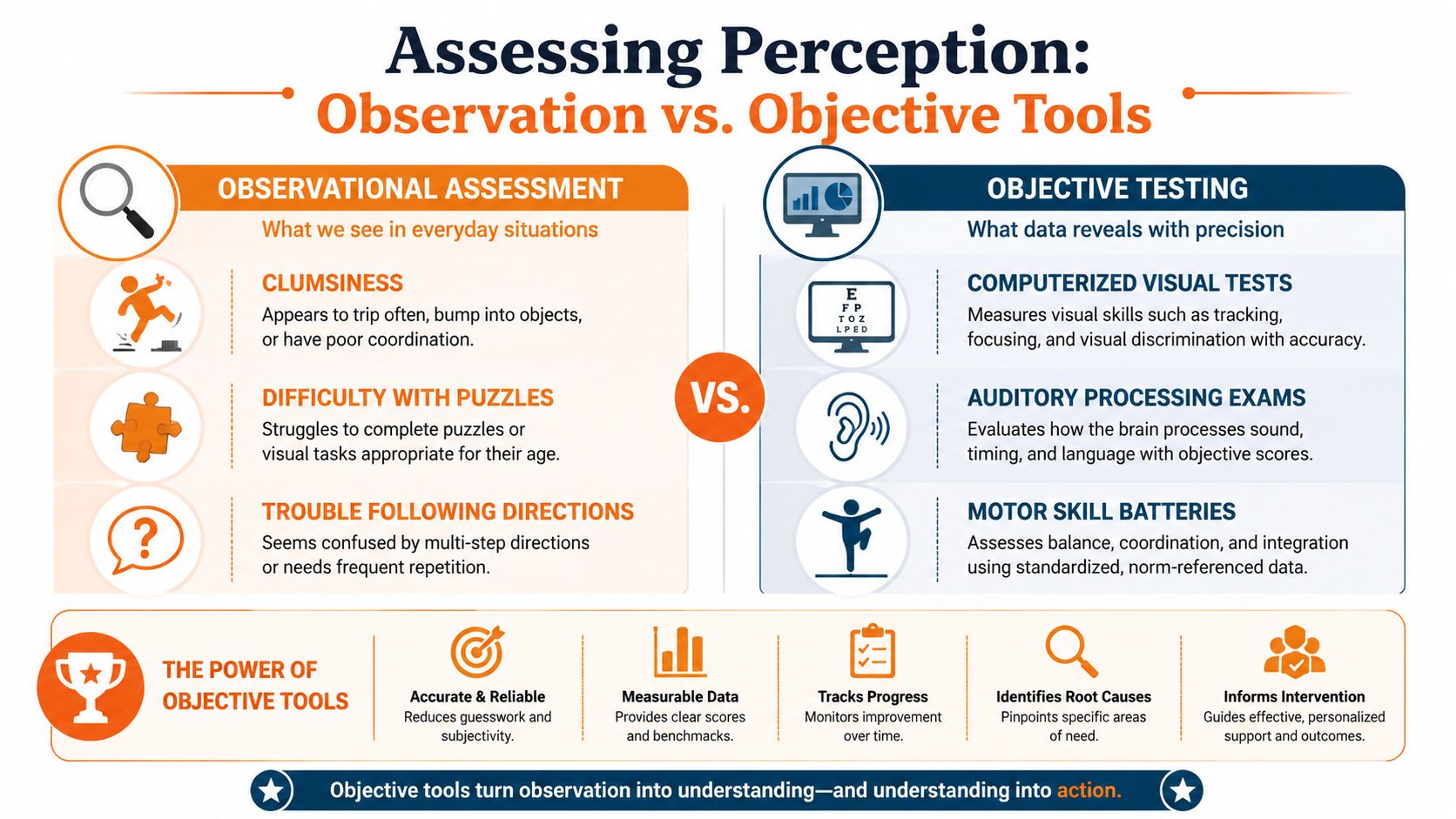
Observation versus structured testing
Here's the practical difference:
Approach | What it can show | What it can miss |
|---|---|---|
Informal observation | Real-world patterns, behaviour, context | Specific subskills and subtle dissociations |
Structured testing | Measurable strengths and weaknesses | Some day-to-day nuance if used alone |
A child who avoids puzzles may have visual-perceptual trouble, spatial trouble, motor planning trouble, or frustration from repeated failure. You won't know which one unless the assessment separates them.
Why subskills matter
The Loewenstein Occupational Therapy Cognitive Assessment (LOTCA-II) does exactly that. It separates the Perceptual area into Visual Perception (4 items), Spatial Perception (3 items), and Motor Praxis (3 items), allowing clinicians to pinpoint specific deficits for targeted rehabilitation (LOTCA-II overview).
That split is clinically useful. “Perception” is too broad to guide intervention by itself.
A practical sequence often looks like this:
Start with basic health questions: Rule out vision or hearing issues that could distort the picture. When visual concerns are part of the story, this guide to the importance of comprehensive eye exams is a helpful reminder that cognitive interpretation and eye health both matter.
Look at everyday function: Can the person organise space on a page, move through a room, match shapes, or imitate movement?
Use a structured profile: Tools that separate sensory and perceptual features can prevent overgeneralising. For some children, a Sensory Profile using Dunn's framework can add useful context about how sensory patterns affect participation.
Practical rule: If the intervention plan wouldn't change based on the result, the assessment is too vague.
Actionable signs worth documenting
Instead of writing “poor perception,” document what happens:
Copies letters with uneven spacing
Gets lost in cluttered worksheets
Misjudges doorways or stairs
Recognises objects better when touched than when seen
Needs extra time to interpret diagrams or visual scenes
That level of detail leads to better referrals, clearer goals, and more meaningful follow-up.
Tracking Perception for Better Care with Objective Tools
A one-time snapshot is useful. It's often not enough.
Perceptual performance can shift with fatigue, stress, medication effects, developmental change, recovery, and environmental demands. If you only test once, you may miss patterns that matter for care planning.
Why repeatable digital measures help
The Integrated Cognitive Assessment (CGN_ICA) is a 5-minute computerized tool that measures cognitive performance by combining speed and accuracy of visual processing. Unlike traditional 15-30 minute exams, this micro-monitoring approach eliminates learning bias and is language-independent, enabling frequent, precise tracking (CGN_ICA study details).
That model is especially relevant for perception because timing and accuracy both matter. Someone may eventually get the answer right, but only after a long delay or with inconsistent performance. In daily life, those delays can affect reading fluency, navigation, safety, and communication.
What clinicians and programmes can do with this information
Repeated objective tracking helps teams answer better questions:
Is the person improving, or just becoming familiar with the task?
Does performance drop at certain times of day?
Are therapy changes reflected in measurable processing differences?
Does the pattern support referral for deeper evaluation?
For programmes that need integrated cognitive data, cognitive assessment tools can support a more structured workflow than narrative notes alone. One example is Orange Neurosciences, which provides objective cognitive profiles that include perception alongside attention, memory, executive function, processing speed, and eye-hand coordination. In practice, that means teams can compare patterns over time instead of relying only on impression.
Good care improves when the team can measure change, not just describe concern.
This is also where digital tools can help families and educators. They don't replace clinical judgement. They make that judgement more informed.
Building a Stronger Perceptual Foundation
Perception is not merely “using the senses.” It's the brain's organised effort to build meaning from incoming information.
That shift in understanding changes how we respond. Instead of asking why a child isn't trying, we ask whether they're misreading space, form, sound, or context. Instead of treating confusion as a single symptom, we look at the steps between sensation and recognition. Instead of relying on broad labels, we identify specific patterns that can be supported.
What to carry forward
A few ideas are worth keeping in mind:
Perception is active: The brain predicts, compares, and interprets.
Perception is specific: Visual, spatial, and praxis-related skills can differ sharply.
Perception is measurable: Care improves when concerns are tracked objectively.
Perception is clinically relevant: It affects learning, mobility, independence, and quality of life.
If you've been asking what is perception because a child, parent, student, or patient seems bright but inconsistent, your instinct is worth trusting. These patterns are real, and they can be explored more precisely than many people realise.
The next practical step is simple. Move from broad concern to targeted assessment. Use observations well, but don't stop there. Look for tools that separate subskills, support follow-up, and help your team make decisions based on data rather than guesswork.
If you want a clearer picture of perceptual strengths and weaknesses, visit Orange Neurosciences. The platform offers objective cognitive assessment and tracking that can help clinicians, educators, and families decide what needs closer evaluation, what should be supported first, and how progress is changing over time. You can also contact the team through the website to learn how their tools fit into clinical, educational, or rehabilitation workflows.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation