Understanding Dementia in Mandarin: Clinician's Guide

A family physician in Vancouver or Toronto sees this often. An adult daughter brings in her mother, a Mandarin-speaking elder who has become quieter, repeats herself, and has stopped managing familiar routines. The daughter says it's probably stress or normal ageing. The physician isn't convinced, but the usual cognitive script doesn't fit. The patient is more comfortable in Mandarin, the family is hesitant, and the test materials on hand were built for someone else.
That's the starting point for dementia in Mandarin. The problem usually isn't a single missed symptom. It's a chain of small mismatches: the wrong term, the wrong interpreter set-up, the wrong assumptions about education, and the wrong screening tool. By the time everyone realises those mismatches matter, valuable time has already gone.
Clinicians and families both feel that friction. So do care planners. For families trying to organise support around a parent's changing cognition, finances, and long-term care, practical frameworks can help. Resources such as Everglow's expert aged care guide are useful because dementia care decisions rarely stay confined to the clinic.
The Unspoken Gap in Cross-Cultural Dementia Care
In clinic, the first barrier often looks deceptively simple. A patient answers politely, smiles, and lets the adult child do most of the talking. If you don't work regularly with cross-cultural assessment, that can look like agreement or preserved function. Sometimes it's neither. Sometimes it's deference, shame, or fear of saying the wrong thing in a second language.

The clinical risk is obvious. If the patient's strongest language isn't the language of assessment, you're no longer testing memory alone. You're testing hearing, comprehension, acculturation, educational exposure, and comfort with the examiner. That's why I treat language of assessment as a diagnostic variable, not an administrative detail. A useful starting reference is this discussion of the language of assessment in neuropsychology.
A second problem is resource quality. Fewer than 15% of dementia resources are linguistically and culturally validated for Cantonese or Mandarin speakers in California, and 42% of Chinese-speaking seniors with cognitive symptoms remain undiagnosed because of language barriers and lack of trusted screening (PMC review on culturally adapted dementia resources). That's not a minor service gap. It changes who gets identified, who gets referred, and who gets left in a grey zone.
What this looks like in practice
A familiar example is the family that reports “memory is fine” but mentions that the elder no longer takes the correct bus, mismanages medications, or gets lost in a familiar Chinese supermarket. Those aren't soft clues. They're functional warning signs.
Another example is the patient who performs poorly on a translated English screen, then appears “globally impaired” on paper. In reality, the test may have overloaded literacy, cultural knowledge, or unfamiliar task demands.
Practical rule: If the assessment language isn't the patient's dominant language, treat every low score cautiously until you've separated cognitive impairment from language and cultural load.
What works is slower, more deliberate triage. Ask who noticed the change first. Ask in which language the problem appears most clearly. Ask whether decline shows up in finances, navigation, medications, cooking, social reciprocity, or managing WeChat messages. Those examples are concrete enough for families to answer and clinically useful enough to guide next steps.
Decoding Dementia Terminology in Mandarin
The words you choose can determine whether a family leans in or shuts down.
In Mandarin, the older term 老年痴呆 (lǎonián chīdāi) has a harsh tone. Families may hear “senile foolishness” or something close to madness, not a medical condition. The more appropriate term in modern clinical conversation is 失智症 (shī zhì zhèng). It's more neutral and much easier to use in discussions about assessment, safety, and care planning.
Why wording changes the whole interview
If a clinician or interpreter uses the older term too early, families may become defensive. They may deny symptoms, minimise risk, or insist the elder is just tired. That reaction isn't always resistance to care. Often it's resistance to shame.
By contrast, when you use 失智症, frame it as a condition affecting memory, thinking, and daily function, and keep the conversation anchored to support needs, families are more likely to stay engaged.
Here's a quick reference that helps in practice.
Mandarin Dementia Terminology Compared
Term (Characters) | Pinyin | Literal Translation | Clinical/Cultural Context |
|---|---|---|---|
失智症 | shī zhì zhèng | loss of intellect or wisdom disorder | Preferred modern medical term. More neutral, less stigmatising, better for clinical interviews and family education. |
老年痴呆 | lǎonián chīdāi | old-age foolishness or senility | Older term with strong stigma. Can imply incompetence, foolishness, or social disgrace. Best avoided in sensitive discussions. |
阿茲海默症 / 阿尔茨海默病 | ā zī hǎi mò zhèng / ā ěr cí hǎi mò bìng | Alzheimer's disease | Useful when discussing a specific diagnosis, especially if the family already recognises the disease name from media or prior care. |
血管性失智症 | xuèguǎn xìng shī zhì zhèng | vascular dementia | Important when the history suggests stroke, hypertension, diabetes, gait change, or executive dysfunction. |
Phrases that preserve dignity
Try phrasing the concern around function rather than labels.
Instead of leading with diagnosis, ask whether the person has had “changes in memory or thinking that affect daily life”.
Instead of asking if the person is confused, ask whether tasks that used to be routine now require more help.
Instead of arguing about normal ageing, ask what has changed compared with the person's own baseline.
“We're not trying to label your parent. We're trying to understand what has changed, what remains strong, and what support would help.”
That wording matters. It respects the elder, lowers the emotional temperature, and gives interpreters language that travels better across settings.
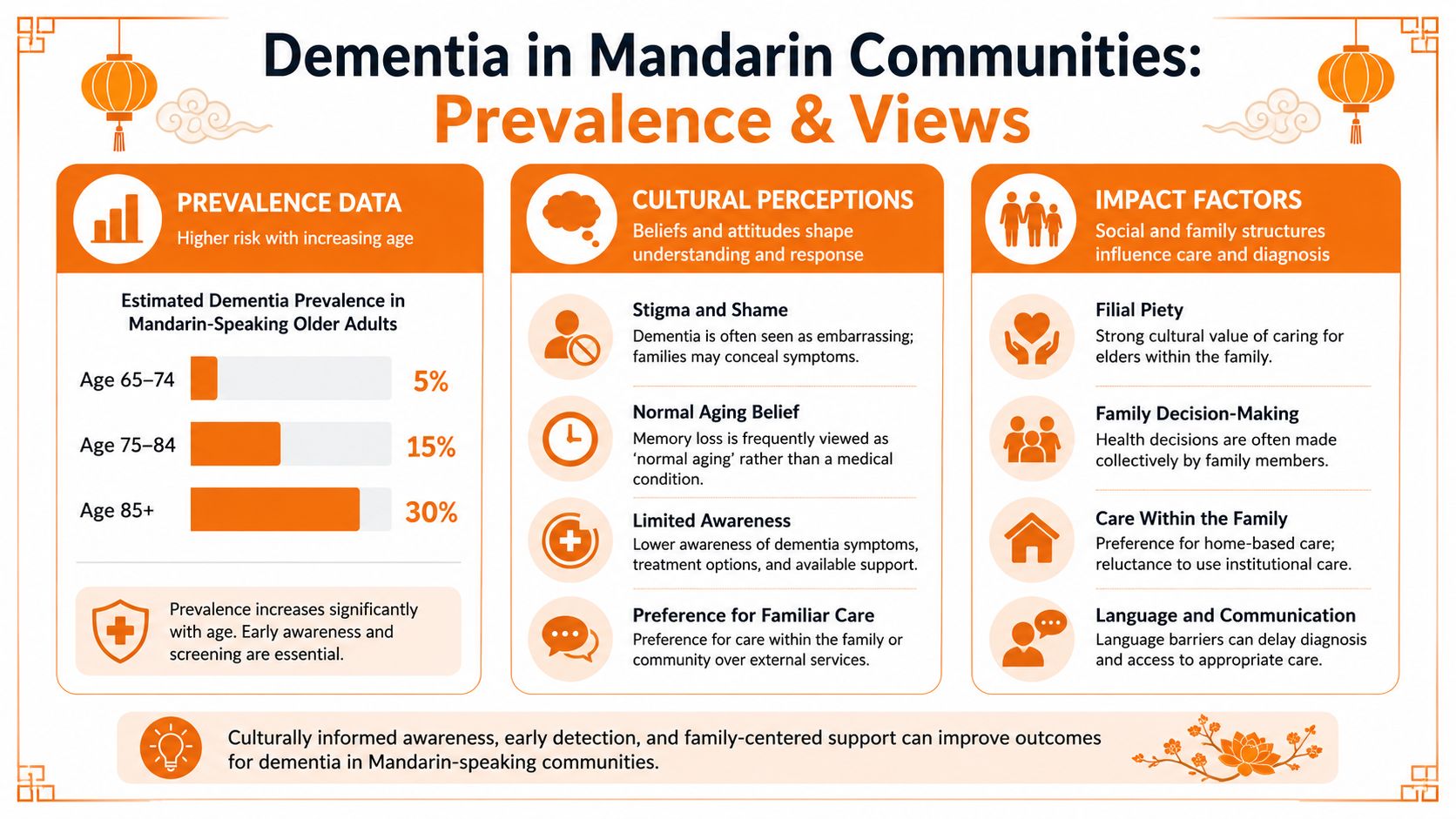
Prevalence and Cultural Views in Mandarin Communities
The epidemiology matters, but numbers alone won't help you unless you connect them to family decision-making.
In China, the overall weighted prevalence of dementia among adults aged 60 and older was 4.22%, with age acting as a dominant risk factor. The same national survey also found that daily tea consumption, regular exercise, and frequent social and intellectual activities were associated with lower risk (national dementia survey in China). For clinicians working with Mandarin-speaking communities in North America, that combination is instructive. Risk rises with age, but the family conversation shouldn't be framed as hopeless or passive.
How cultural views delay recognition
Many families don't come in saying, “I think this is dementia.” They come in saying, “She's older now,” or “He doesn't want to bother us,” or “He's become more quiet since retirement.” In Mandarin-speaking households, three themes come up repeatedly.
Normal ageing beliefs: Memory change may be seen as an ordinary part of later life rather than a medical issue.
Filial responsibility: Adult children may feel they should manage privately and avoid exposing a parent to embarrassment.
Burden avoidance: Elders may hide symptoms because they don't want to trouble their children.
These beliefs don't mean the family is indifferent. Usually the opposite is true. The family is trying to protect dignity, but that protection can delay diagnosis.
What families can do that actually helps
When I'm speaking with caregivers, I don't start with abstract prevention language. I ask about routines.
A practical example: an older adult who has stopped attending mahjong, church, temple, or local senior gatherings may lose more than social contact. They may also lose a regular source of cognitive stimulation and real-world monitoring. Another example is the elder who still drinks tea daily but has become sedentary and isolated. Tea alone won't offset the functional consequences of inactivity and withdrawal.
The most useful prevention conversation is often the simplest one: keep the person moving, socially engaged, and mentally involved in meaningful routines.
There's also an encouraging point for bilingual families. Bilingual individuals are diagnosed with dementia an average of 3.3 years later than monolinguals, and Alzheimer's disease specifically is delayed by 4.2 years, although bilingualism doesn't significantly reduce overall odds of developing the disease (review on bilingualism and dementia timing). That doesn't mean bilingualism prevents dementia. It does mean many Mandarin-English speakers may function well for longer before symptoms become clinically obvious. Families sometimes misread that reserve as proof that nothing serious is happening. It's better understood as a reason to pay close attention to subtle decline.
Overcoming Key Challenges in Cognitive Assessment
A translated test isn't automatically a valid test.
That's the mistake I see most often in dementia in Mandarin assessments. Clinicians may use a familiar screen, translate it on the fly, and assume they've preserved the construct. They haven't. Once you alter wording, cultural references, educational load, or response expectations, you may be measuring something different.

Why direct translation often fails
Some items depend heavily on alphabetic literacy, formal schooling, or Western cultural familiarity. Others rely on speeded verbal output that can be distorted by interpreter pacing, dialect differences, or anxiety. If the patient had limited formal education, a “poor” score may reflect test fit as much as impairment.
This is why a review of common cognitive screening tests for dementia should always be paired with a language and education analysis before you interpret the result.
Here are the trade-offs clinicians need to weigh:
Interpreter use helps access, but it can alter timing and nuance. That matters when the task depends on rapid comprehension or exact phrasing.
Family interpretation may feel convenient, but it can contaminate the sample. Relatives often simplify, prompt, soften errors, or answer for the patient.
Low education can mimic cognitive disorder on paper. If you ignore schooling history, you risk overcalling impairment.
Highly educated bilingual patients can mask decline. Their reserve may keep basic screens deceptively normal while executive inefficiencies are already emerging.
The vascular dementia issue clinicians can't miss
Subtype matters. For Mandarin-speaking older adults, vascular dementia accounts for a significantly higher proportion of cases, around 35% to 40%, compared with 20% to 25% in Caucasian populations. Hypertension and diabetes are key modifiable risk factors (study on dementia subtype patterns in Chinese populations).
That shifts the clinical lens. If you expect the classic amnestic presentation every time, you'll miss patients whose first clear problems are slowed processing, mental flexibility, planning, sequencing, or divided attention.
A practical example: a patient may still recall parts of a recent conversation but can no longer organise a multistep meal, manage blood pressure tablets correctly, or shift between tasks without becoming stuck. Another may appear less forgetful than expected, yet shows poor judgement in finances and trouble following a route with multiple turns.
Don't anchor on memory alone. In many Mandarin-speaking elders, executive change and vascular burden deserve equal attention early in the workup.
What doesn't work is relying on a single brief score and declaring the picture settled. What works is pattern recognition. Look at vascular history, functional change, educational background, language dominance, and whether the observed deficits fit the subtype you suspect.
Validated Mandarin Screening Tools and Resources
Once you've recognised the assessment pitfalls, the next step is choosing tools that were built or validated for Mandarin speakers.
The strongest brief options at present are the Mandarin versions of the Addenbrooke's Cognitive Examination Revised and ACE-III. In a 2024 study, Mandarin-specific cognitive tests showed 93.5% sensitivity and 85.6% specificity for detecting dementia in Chinese-speaking older adults, with the Addenbrooke's measures identified as especially effective. These tools also correlated strongly with English-language tests and novel blood-based Alzheimer's biomarkers (2024 study on Mandarin cognitive tests).
How to use the right tool for the right question
Not every patient needs the same entry point. Here's a practical way to think about it.
Use a validated Mandarin screen when the patient is clearly most comfortable in Mandarin and you need a brief, clinically grounded first pass.
Prioritise a broader neuropsychological referral when the screen result doesn't match the family's functional concerns, especially in highly educated or bilingual patients.
Be cautious with language-heavy tasks if hearing, literacy, or dialect mismatch is muddying the picture.
Look beyond memory totals when vascular burden, diabetes, or blood pressure history suggests frontal-subcortical involvement.
If you need families to understand why one test may be preferable to another, it helps to compare the purpose of different instruments plainly. A general explainer on the Montreal Cognitive Assessment test format and limitations can be useful for that conversation, particularly when families arrive asking for “the standard memory test” without realising how language-sensitive some tools are.
What's emerging and what to do with it now
There's also credible movement toward speech-based detection. A 2023 study using Mandarin speech analysis during picture description tasks achieved 92.04% accuracy in Alzheimer's detection and a mean absolute error of 9% in predicting clinical dementia rating scores within Mandarin-speaking cohorts, as reported within the same PubMed-indexed review summary on Mandarin assessment advances. That's promising because speech captures more than recall. It reflects fluency, lexical access, organisation, and self-monitoring.
For now, I'd treat speech analysis as an adjunct, not a standalone answer. It may become especially useful when in-person specialist access is limited or when repeated low-burden monitoring is needed.
Families often ask for trustworthy plain-language materials between appointments. In that setting, curated tools such as Z Audiology dementia resources can support early conversations, provided they're used as education rather than diagnosis.
What works best is a layered toolkit. Start with the patient's strongest language, choose a validated instrument, and escalate when the clinical story and the score don't agree.
Effective Communication Strategies for Clinicians and Caregivers
A good assessment can still fail if the conversation around it is clumsy.
The goal isn't to sound delicate. It's to protect dignity while gathering accurate information. In dementia in Mandarin care, blunt phrasing often triggers shame, concealment, or family gatekeeping. Careful wording tends to produce better disclosure.

Phrases that usually work better
When possible, speak through a qualified interpreter and address the patient first, not just the adult child.
Try phrasing like this:
To introduce testing: “We use these tasks to understand changes in attention, memory, and daily thinking skills.”
To ask about function: “What has become harder at home that used to feel routine?”
To explore safety: “Have there been any recent problems with medications, finances, cooking, or getting to familiar places?”
To frame next steps: “The purpose is to understand what support will help now, not to take away independence unnecessarily.”
This style aligns well with client-centered care principles in cognitive health, especially when the family is involved but the elder's dignity still needs to remain central.
What clinicians and caregivers should avoid
Some communication habits reliably derail the encounter.
Don't force confrontation. Saying “Your mother has dementia” before completing the workup may shut the family down.
Don't let relatives answer every question. Family history is valuable, but you still need the patient's own language, tone, and effort.
Don't use children as interpreters. It distorts clinical content and can be distressing for everyone involved.
Don't ignore non-cognitive symptoms. Families may cope better with practical guidance about sleep, continence, irritability, or mobility than with abstract labels. For example, aged care advice on incontinence can help when families are overwhelmed by daily care needs that they didn't expect to accompany cognitive decline.
Respect is not a soft extra in these encounters. It's the condition that makes accurate disclosure possible.
A useful habit is to end each appointment with one sentence directed to the patient, one to the family, and one shared next step. That simple structure reduces confusion and signals partnership.
Building a Referral Pathway and Next Steps
By the time a Mandarin-speaking patient reaches specialist care, the family has often already spent months trying to interpret what they're seeing. A clear pathway reduces that drift.
In California's Orange County, the prevalence of Alzheimer's disease and related dementias is 19.8%, which underscores how important organised care pathways are in regions serving large Chinese-speaking communities (California ADRD prevalence report). High regional burden means primary care, geriatrics, neurology, rehabilitation, and community supports all need a common workflow.
A practical referral sequence
Recognise the language issue early. Determine the patient's dominant language, dialect comfort, literacy history, and who is currently reporting change.
Clarify the everyday problem. Ask about navigation, medication use, shopping, cooking, financial handling, and social withdrawal. Families often reveal the decisive clues here.
Use a culturally appropriate baseline. Start with a brief cognitive measure suited to the patient's language profile and educational background.
Escalate to validated Mandarin screening when indicated. If concerns persist, use a Mandarin-validated tool rather than a casual translation of an English screen.
Refer for formal diagnosis when the picture is complex. Neurology, geriatric psychiatry, geriatrics, or neuropsychology may be the right next stop depending on the differential.
Connect the family to practical support. Education, caregiver coaching, safety planning, and culturally acceptable community resources matter as much as the diagnosis itself.
What a strong handoff includes
A good referral is specific. It should state the patient's preferred language, whether an interpreter is required, estimated education level, vascular risk factors, and the exact functional changes prompting concern. If you merely write “memory loss,” the next clinician starts almost from zero.
For families searching locally, a regional directory such as this guide to finding neuropsychology services can help them understand what kind of specialist they may need and what that assessment is likely to involve.
The bigger point is simple. Dementia in Mandarin isn't solved by translation alone. It requires accurate terminology, culturally safer interviewing, validated instruments, and a referral path that respects both the patient's language and the family's decision-making style.
If you're building a more reliable pathway for multilingual cognitive assessment, visit Orange Neurosciences. The platform offers rapid, objective cognitive profiling that can help clinicians and families decide when further evaluation is warranted, especially when language and culture make first-line assessment more complicated.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation