Cognitive Screening Tests for Dementia A Clinician's Practical Guide
Feb 11, 2026

Cognitive screening tests for dementia are quick, practical assessments clinicians use to spot potential trouble with a person's memory, thinking, and reasoning. These tools, like the well-known MoCA or Mini-Cog, aren't designed to give a final diagnosis. Instead, they’re an essential first step—a way to flag individuals who might need a closer look. For instance, if a patient’s spouse mentions they are repeatedly asking the same questions, a quick screening can provide an objective measure to guide your next steps.
Why Early Cognitive Screening Is Essential for Dementia Care

Picture this: during a routine check-up, a patient's family casually mentions some small, easily dismissed memory lapses, like forgetting appointments or struggling to find the right words. For a busy clinician, these subtle remarks are critical signals. This is exactly where cognitive screening tests for dementia come in, helping to turn these subjective worries into concrete data you can act on.
Think of these brief assessments as a smoke detector for cognitive change. A smoke detector can't tell you what caused the fire or how to put it out, but it gives you that crucial early warning to take action. In the same way, a screening test helps establish a cognitive baseline, ideally long before any significant decline becomes obvious, giving you a starting point for all future care.
The Proactive Advantage in Patient Management
Catching potential issues early with screening gives clinicians and families a massive head start. It opens the door for better long-term planning and management, which is absolutely fundamental to improving patient outcomes down the road.
Here are the actionable benefits of getting ahead of the curve:
Establishing a Baseline: A screening test gives you an objective snapshot of a patient's cognitive function right now. Actionable Insight: Use this baseline to track changes over time. A drop from a MoCA score of 28 to 25 in one year is a significant flag, even if both scores are "normal."
Facilitating Timely Interventions: Early identification allows for lifestyle modifications—like changes in diet, exercise, and social engagement—that may help slow cognitive decline. Actionable Insight: Refer patients with borderline scores to nutritionists or physical therapists to proactively manage risk factors.
Improving Patient and Family Planning: An early heads-up gives patients and their families precious time to make important legal, financial, and healthcare decisions while the patient can still be fully involved. Actionable Insight: Provide families with a checklist for advance care planning and local resources for legal aid.
Connecting to Support Services: Clinicians can connect families with community resources, support groups, and educational materials much earlier, which can significantly reduce caregiver stress and improve everyone's quality of life.
A cognitive screening test is not about delivering a definitive diagnosis. It's about identifying risk and initiating a conversation, creating a pathway for informed, compassionate, and timely care that respects the patient's future autonomy.
Transforming Ambiguity into Action
Without a formal screening process, concerns about memory often get stuck in a grey area of "watchful waiting." This passive approach can mean missed opportunities for intervention.
For instance, if a patient scores slightly below the expected range on a test, it prompts a clear next step. Maybe that’s scheduling a follow-up screening in six months, or perhaps it means a referral for a full neuropsychological evaluation. This simple step turns vague worries into a clear, manageable clinical pathway. You can learn more about picking up on the early signs in our detailed guide on what is cognitive decline. Ultimately, this structure benefits everyone involved in the patient's care.
A Look at Traditional Pen and Paper Screening Tools
For decades, pen-and-paper tests have been the bedrock of initial dementia screening. They’re familiar, don't require expensive equipment, and can be done just about anywhere. It's a straightforward approach that has served clinicians well.
But here’s the thing: not all of these tools are interchangeable. Each was designed with a specific job in mind, and they shine in different clinical situations. Knowing which instrument to pull out of your toolkit is the first step toward a more accurate and helpful assessment for your patient.
Let's move past the textbook definitions and get into what really matters—how four of the most common screening tests work in the real world, what they’re good at, and where they fall short.
Mini-Mental State Examination (MMSE)
The MMSE is probably the most famous cognitive screener on the planet. If you've worked in this field, you've almost certainly used it. It gives a broad overview by testing orientation, memory, attention, and language.
It’s most powerful when you’re looking at moderate to severe cognitive impairment. Practical Example: For a patient already diagnosed with Alzheimer’s disease, using the MMSE annually is a solid, practical choice for tracking how their condition is progressing over time.
Because it’s so well-known, most clinicians can administer and score it in their sleep. It's also quick, usually taking just 7-10 minutes. The biggest drawback? The MMSE has a serious "ceiling effect." Someone with a high level of education or in the very early stages of impairment can ace the test, giving you a false sense of security. It’s also notoriously swayed by a person's educational and cultural background.
To see just how it compares to newer tools, check out our in-depth look at the MoCA vs MMSE.
Montreal Cognitive Assessment (MoCA)
The MoCA was developed specifically to catch what the MMSE often misses. Its superpower is detecting mild cognitive impairment (MCI).
The MoCA casts a wider net, digging deeper into things like executive function and attention—two areas that often show the first signs of trouble. It uses more complex tasks like the clock-drawing test, trail making, and verbal fluency exercises to challenge those higher-level brain processes.
Actionable Insight: When a family describes subtle but persistent changes in their loved one’s ability to plan or solve problems—like struggling with a familiar recipe or managing finances—the MoCA is far more likely to pick up on those deficits than the MMSE.
It takes a little longer, around 10-15 minutes. While its sensitivity is a huge plus, it also means you might see more false positives. It's critical to interpret the MoCA score within the full clinical picture of the patient, not in isolation.
Mini-Cog
Time is everything in a busy primary care clinic, and that’s where the Mini-Cog comes in. This test is a model of efficiency, taking only 3-5 minutes from start to finish.
It’s brilliantly simple, combining just two tasks:
Three-Word Recall: A basic memory challenge.
Clock Drawing: A surprisingly complex task that taps into visuospatial skills and executive function.
Practical Example: You can administer the Mini-Cog while taking a patient's vitals during an annual physical. If they struggle to recall the words or draw the clock correctly, you have an immediate, objective reason to schedule a longer follow-up appointment for a more comprehensive test like the MoCA. This quick-fire combination is incredibly effective for its brevity. A huge advantage is that it’s far less influenced by a person's language or education level, making it a practical first-line screener for almost any patient.
The trade-off for speed is detail. The Mini-Cog is a blunt instrument; it tells you there might be a problem, but not much more. A failed Mini-Cog is a clear signal that it’s time to bring out the more comprehensive tests.
Saint Louis University Mental Status (SLUMS) Exam
The SLUMS exam is another fantastic option for identifying milder cognitive problems, fitting neatly between the rapid Mini-Cog and the more intensive MoCA. It takes about 10-15 minutes and covers similar ground, including attention, memory, and executive function.
What makes the SLUMS stand out is its clever scoring system. It uses different cut-off scores based on the patient's level of education—for example, whether they finished high school or not. This simple adjustment goes a long way toward reducing the educational bias that plagues other tests.
This built-in correction makes the SLUMS a much fairer screening tool for clinics serving people from diverse educational backgrounds. Ultimately, the right test depends entirely on your goal. Are you screening a busy waiting room, investigating subtle memory complaints, or tracking a known condition? Each scenario has a tool that fits just right.
At-a-Glance Comparison of Common Screening Tests
To make the choice a little easier, here’s a quick-reference table summarizing the key features of these widely-used pen-and-paper cognitive screening tools.
Test Name | Primary Focus | Avg. Time | Key Advantage | Key Limitation |
|---|---|---|---|---|
MMSE | Moderate to severe impairment | 7-10 min | Widespread familiarity, quick to administer | High ceiling effect, influenced by education |
MoCA | Mild cognitive impairment (MCI) | 10-15 min | High sensitivity for early-stage changes | Higher rate of false positives if not contextualized |
Mini-Cog | Rapid screening for cognitive issues | 3-5 min | Very fast, low educational/language bias | Lacks diagnostic detail, only a coarse screen |
SLUMS | Mild cognitive and neurocognitive issues | 10-15 min | Adjusts scoring for education level | Less known than MMSE or MoCA, training needed |
This table can act as a quick mental checklist when you're deciding which screener is most appropriate for the patient in front of you, balancing the need for speed, sensitivity, and fairness.
How to Interpret Screening Results and Guide Next Steps
A score from a cognitive screening test is just one piece of a much larger puzzle. Think of it as a single frame from a movie; it’s a useful snapshot, but it certainly doesn’t tell the whole story. To really get at what that number means, you have to place it within the full context of the patient's life.
This means looking beyond the score to consider crucial factors like their educational background, cultural context, and any sensory impairments they might have. For example, a lower score for a patient with hearing loss could simply reflect difficulty understanding the instructions, not a true cognitive deficit. The goal is always to see the person, not just the number.
Navigating Ambiguity: A Practical Case Study
Let's walk through a common and often tricky scenario. Imagine your patient is a 72-year-old retired professor with a PhD, and she scores a 25 on the MoCA. This score is technically just below the typical cut-off of 26, landing it in a borderline grey area.
So, what do you do?
First, resist the knee-jerk reaction. It’s tempting to either dismiss the score because of her high intellect or, conversely, immediately refer her for extensive testing. Neither is the right first step.
Context is everything. For someone with such a high cognitive reserve, a score of 25 could be a significant red flag. Her baseline is likely much higher than the average person's. A score that might be "normal" for someone else could represent a meaningful decline for her.
Dig deeper. Now is the time for a careful clinical interview. Ask her and her family about specific changes. Is she having trouble with complex tasks she used to handle with ease, like managing finances or planning multi-step projects? These subjective reports are suddenly just as important as the test score.
This case highlights a core principle: a borderline score in a highly educated individual warrants more attention, not less. It’s a signal to investigate further, not to simply wait and see. For a deeper dive into the nuances of scoring, you can explore our guide on MoCA score interpretation.
Communicating Findings with Empathy and Clarity
Discussing the results of cognitive screening requires a delicate touch. Patients and their families are often anxious, and your delivery can either dial up their fear or empower them with a clear plan.
Start by framing the result correctly. Explain that the screening isn't a diagnostic test for dementia but a tool to check on their cognitive health—a bit like how a high blood pressure reading doesn't automatically mean a heart attack is imminent, but it does mean it's time to pay closer attention and take proactive steps.
The most compassionate and effective approach is to reinforce that this is a collaborative process. Frame the next steps not as a verdict, but as a shared plan to understand what's happening and how to best support their brain health moving forward. Actionable Insight: Use phrases like, "This score gives us a reason to look a bit deeper. Let's schedule a follow-up test in six months to see if there's a pattern, and in the meantime, let's talk about brain-healthy habits."
Deciding on the Next Steps
Once you've interpreted the score in context, the path forward usually leads to one of two places. The decision hinges on the complete clinical picture—the score itself, the patient's history, and any reports from caregivers.
Watchful Waiting and Repeat Testing: This is a sound approach when a borderline score appears in a patient with no functional complaints or other worrying signs. The plan needs to be concrete: schedule a follow-up screening in 6 to 12 months, using the exact same tool to create a direct comparison. This longitudinal view is incredibly powerful for detecting subtle but consistent decline over time.
Referral for a Full Evaluation: A referral to a specialist for a comprehensive neuropsychological evaluation becomes necessary when:
The screening score is significantly low.
The patient shows a clear decline from a previous test.
There are reports of significant functional impairment in daily life, regardless of the score.
The clinical picture is complex and simply needs a specialist's diagnostic expertise.
Making a decisive referral gives the patient access to a definitive diagnosis and a more detailed care plan. Your role in the screening process is to identify that risk and open the door to that next level of care.
The Shift to Digital and AI-Powered Cognitive Assessments
For years, the standard for cognitive screening has been pen-and-paper tests. While they've served a purpose, they come with a host of familiar challenges: long wait times for specialist referrals, scoring that can vary from one clinician to the next, and biases baked in by a person's culture or education. Technology is finally stepping in to bridge these gaps, offering a more objective, efficient, and equitable path forward.
This isn't about replacing a clinician's expert judgment. Far from it. It's about augmenting that expertise with powerful tools that offer much deeper insights. Think of a traditional test as a single snapshot of a patient's cognitive health. A digital assessment, on the other hand, is more like a high-definition video, capturing nuanced performance over time and across multiple cognitive domains.
Overcoming the Limitations of Traditional Screening
Digital platforms are designed to solve the very problems that have long frustrated clinicians. They offer standardized administration and automated, objective scoring, which takes the guesswork and variability out of the process.
This digital-first approach directly dismantles some of the biggest barriers to effective care. For example, AI-driven tools can deliver assessments in a patient's native language without needing a live interpreter, removing potential bias and giving you a truer picture of their cognitive abilities. Our guide on online cognitive assessments dives deeper into how these modern tools are structured for today's clinical needs.
The real power of digital cognitive screening tests for dementia lies in their ability to deliver a multi-domain cognitive profile quickly and objectively. This allows clinicians to move from a simple pass/fail score to a detailed map of a patient's cognitive strengths and weaknesses.
These platforms can also integrate seamlessly into existing electronic health records (EHR). This simple step makes cognitive data an accessible, standard part of the patient's overall health profile, streamlining your workflow and making it infinitely easier to track cognitive changes with precision over time.
Speed, Objectivity, and Data-Driven Insights
The sheer efficiency of digital assessments is a game-changer for any busy practice. While traditional tests held a 46.58% share of the healthcare cognitive assessment market in 2026, they are quickly being outpaced by AI-powered alternatives. Why? These new tools can slash administrative costs by about 95% and deliver detailed results in under 30 minutes.
This directly tackles the notorious six-month waitlists for full neuropsychological evaluations. For providers in rehab centres or senior living communities, this means faster and smarter triage. Practical Example: An early screening with a tool like Orange Neurosciences' OrangeCheck can flag potential decline in key areas like memory or executive function, giving you a clear, data-backed reason to pursue a full diagnostic workup—or to simply continue monitoring.
This flowchart shows a simplified protocol for how screening results can guide your next steps.
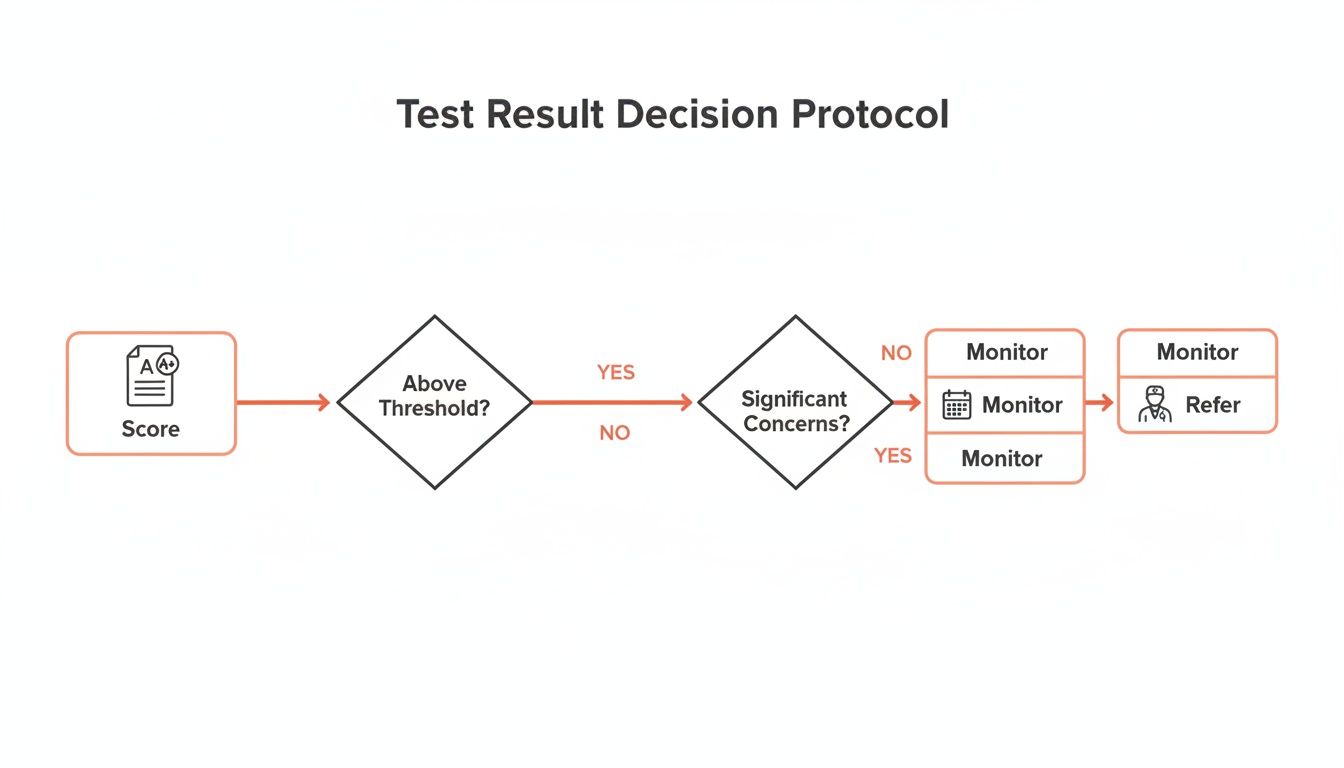
The clear flow from a score to a decision—monitor or refer—is a perfect example of how structured data simplifies and accelerates clinical action.
This rapid, data-rich output empowers you to make more confident decisions, much sooner. For those interested in taking data interpretation a step further, exploring how AI and machine learning for predictive analytics in healthcare can enhance this process is a worthwhile read. It’s all about building a more complete and proactive picture of a patient's cognitive health journey.
The move toward digital isn’t just about making things easier; it’s about elevating the standard of care. By providing faster, more objective, and culturally neutral data, AI-powered cognitive assessments equip clinicians to spot potential issues earlier, intervene more effectively, and ultimately improve long-term outcomes for their patients.
Weaving Digital Screening into Your Clinical Workflow
Making the switch from pen-and-paper screening to a digital platform might seem like a big leap, but it’s actually a pretty straightforward move that pays off in efficiency. Modern tools are designed to slot right into your existing routines, not blow them up. The trick is to map out a clear plan, from the moment a patient checks in to when you’re sitting down with their report.
Think of it like swapping an old paper appointment book for a digital calendar. There's a small learning curve, sure, but you'll quickly wonder how you ever got by without the automatic reminders and instant access. The goal here is to make cognitive screening as routine and objective as taking a patient’s blood pressure.
A Sample Workflow in Action
Bringing a tool like OrangeCheck into your practice can be broken down into a simple, repeatable process. This ensures that cognitive data is captured consistently, everyone on your team knows their role, and the results are ready for you to interpret without the administrative headache.
Here’s an actionable plan to implement this in your clinic:
Patient Intake and Setup: When a patient checks in, your administrative staff or a medical assistant can get them started on a tablet or computer in a quiet corner. Actionable Step: Create a one-page instruction sheet for staff to ensure consistent setup for every patient.
Assessment Administration: The patient then works through the self-guided, often game-like assessment. Platforms like Orange Neurosciences use clear instructions and adaptive challenges, and the whole thing usually takes less than 30 minutes.
Automated Scoring and Report Generation: The second the patient finishes, the platform crunches the numbers and generates a comprehensive report covering multiple cognitive domains. This objective profile is sent securely right to the EHR or your clinician portal.
Clinical Review and Decision-Making: During the consultation, you have a detailed, easy-to-read report at your fingertips. You can review objective data on memory, executive function, and attention to guide your conversation and decide on the next steps. Actionable Step: Use the report's visual data to show patients and families which cognitive areas are strong and which need attention, making the conversation more concrete.
This structured approach takes the burden of manual scoring and paperwork off your plate, freeing you up to spend more quality time with your patient.
Going Deeper with Longitudinal Monitoring
One of the most powerful things about digital platforms is their ability to support longitudinal monitoring. Because the tests are standardized and objective, you can have a patient take one every 6-12 months to track cognitive changes with incredible precision. This turns screening from a one-off event into a fundamental part of proactive, ongoing care.
Practical Example: You can see how a patient is responding to a new treatment, monitor their recovery after a stroke or TBI, or catch those subtle declines that might be the very first whisper of a neurodegenerative condition. This steady stream of data gives you a much richer picture of a patient’s cognitive journey and builds a strong foundation for excellent continuity of care in your practice.
The Practical and Financial Side of Things
The business case for going digital is hard to ignore. While neuropsychologists have historically relied on desktop-based assessments—which account for 61.7% of revenues in settings like care homes—the tide is turning. The global cognitive assessment market is projected to hit USD 58.53 billion by 2032, and much of that growth is driven by the sheer efficiency and accessibility of digital tools.
Platforms like OrangeCheck, which are FDA-cleared and available in over 20 languages, get rid of interpreter biases and can slash costs by up to 95% compared to older tests. For clinics in North America, which held a 38.7% market share in 2023, bringing these tools on board is a smart, strategic move to stay ahead of the curve and improve patient outcomes. You can dig into these trends in the cognitive assessment market for more detail.
Adopting a digital workflow isn’t just a tech upgrade. It's a strategic decision to boost your diagnostic confidence, get patients more engaged in their own health, and future-proof your practice for the growing demand for dementia care.
To see how seamlessly this can fit into your own clinic, we invite you to visit our website and request a personalized demo. Discover how Orange Neurosciences can elevate your practice's approach to cognitive screening and dementia care.
Burning Questions About Cognitive Screening
When you're wading into the world of cognitive screening for dementia, questions naturally pop up for clinicians and concerned family members alike. Getting clear, straightforward answers is the first step toward making good decisions and providing the best possible care.
Let's tackle some of the most common questions we hear from people on the front lines. These answers are designed to be practical, helping you connect the dots between the concepts in this guide and what you see in your clinic every day.
How Often Should We Be Screening?
There's no single, magic number here; the right frequency really depends on the individual sitting in front of you.
For patients over 65 with no obvious symptoms or complaints, an annual screen during a regular wellness visit is a great way to establish a baseline. Think of it as a yearly vital sign for the brain.
If someone has known risk factors (like a family history) or is already voicing concerns, you'll want to get a baseline immediately. From there, re-testing every 6 to 12 months is crucial to track any changes over time.
Actionable Insight: Set up an automated reminder in your EHR to prompt for cognitive screening during annual wellness visits for all patients over 65. This ensures it becomes a routine part of proactive care, not an afterthought.
Can Someone Pass a Screening Test but Still Have Dementia?
Absolutely. It happens more often than you might think, especially in the earliest stages of the disease or with people who have a high cognitive reserve. Practical Example: Someone with a PhD or a long career as an accountant has spent a lifetime building mental workarounds. They can often compensate and ace a brief test, even when underlying problems have started to develop.
A screening score is just one piece of the puzzle. It should never be the only thing you rely on. You have to look at it alongside a thorough clinical history, reports from caregivers, and your own observations to see the full picture.
This is a huge reason why more sensitive instruments, like the MoCA, or objective digital assessments are often preferred. They're better at picking up on the quiet, early-stage changes that simpler tests might not catch.
What’s the Difference Between a Screening and a Full Evaluation?
Think of it this way: a screening is like a quick temperature check, while a full evaluation is the complete diagnostic workup that follows.
Screening: This is a quick, 10-15 minute test designed to flag a potential problem. It's an efficient first pass to see who might need a closer look.
Full Neuropsychological Evaluation: This is the deep dive, often taking several hours with a specialist. They use a whole battery of tests to formally diagnose a condition, figure out the specific type of dementia, and map out a detailed care plan.
In a nutshell, cognitive screening tests for dementia are that critical first step. They help us identify who needs to be referred for that deeper evaluation, making sure specialist resources go to the patients who truly need them.
Ready to bring objective, efficient cognitive screening into your practice? Orange Neurosciences offers a powerful digital platform that delivers precise cognitive profiles in under 30 minutes, helping you make faster, more informed decisions for your patients. Request a demo to see how our tools can elevate your approach to dementia care. Learn more at https://orangeneurosciences.ca.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation