A Clinician's Guide to the Rivermead Post Concussion Symptoms Questionnaire
Jan 26, 2026

For clinicians on the front lines of concussion care, the Rivermead Post-Concussion Symptoms Questionnaire (RPQ) is an indispensable tool. It’s designed to do something remarkably important: turn subjective, often confusing patient feelings like dizziness or brain fog into clear, measurable data. This is a crucial step for effective treatment, much like the broader effort involved in recognising the signs of mental health problems.
Why the RPQ is a Cornerstone of Concussion Care
After a head injury, patients can find it incredibly difficult to put their experience into words. Symptoms often feel vague, they come and go, and can be easily brushed aside. The RPQ provides a structured, common-sense framework that captures these feelings, moving clinicians and patients away from guesswork and toward a solid, quantifiable baseline of the post-injury state.
It's less of a diagnostic test and more of a guided conversation. The real power of the RPQ is how it standardizes the way symptoms are reported and, just as importantly, tracked over time. This consistent approach has made it a staple in neurological and rehabilitation settings for a few key reasons.
Creating a Clear Symptom Profile
The main job of the RPQ is to create a detailed snapshot of what a patient is going through. It methodically asks about 16 specific issues—covering everything from headaches and fatigue to irritability and trouble concentrating—making sure nothing important gets missed. This thorough approach helps clinicians grasp the full scope of a patient’s challenges.
Practical Example: A patient might come in saying they just "feel off." The RPQ helps you break that vague feeling down into actionable data:
Are they dealing with moderate headaches (a score of 3)?
Is their sleep disturbance a mild problem (a score of 2)?
Do they have severe sensitivity to light (a score of 4)?
Getting this level of detail is absolutely essential for building a treatment plan that actually fits the individual’s specific needs. You can explore how different tools work together in our detailed guide on the concussion symptom questionnaire.
Validating the Patient Experience
One of the most powerful, and sometimes overlooked, benefits of a tool like the RPQ is how it validates what the patient is feeling. The effects of a concussion are often invisible, which can feel incredibly isolating. When a clinician sits down with a patient and goes through the RPQ, it sends a clear message: your symptoms are real, they matter, and we’re taking them seriously.
This simple act of measurement can be a huge step forward in the recovery journey. It builds trust and opens up the lines of communication between the patient and their care team.
By converting subjective complaints into objective scores, the RPQ builds a bridge of understanding. It allows both the clinician and the patient to see progress, identify setbacks, and make data-informed decisions about the next steps in rehabilitation.
This systematic approach is the foundation of modern concussion management. But subjective symptom data is just one piece of the puzzle. The most complete picture of brain health comes when this information is paired with objective cognitive metrics, giving you a truly robust view of a patient’s recovery.
How to Administer and Score the RPQ
Using the Rivermead Post Concussion Symptoms Questionnaire (RPQ) effectively is about more than just handing a form to a patient. Its real power comes from consistent administration and precise scoring, which helps turn a patient's subjective feelings into objective data points you can actually track over time.
Let's walk through the practical steps to make this tool a reliable part of your clinical work.
The heart of the questionnaire is its 16 items, covering the most common post-concussion symptoms. We're talking about everything from physical issues like headaches and dizziness to cognitive hurdles like poor concentration and emotional shifts like irritability.
This simple flow shows how the RPQ helps translate a patient's internal experience into structured, actionable data that clinicians can work with.
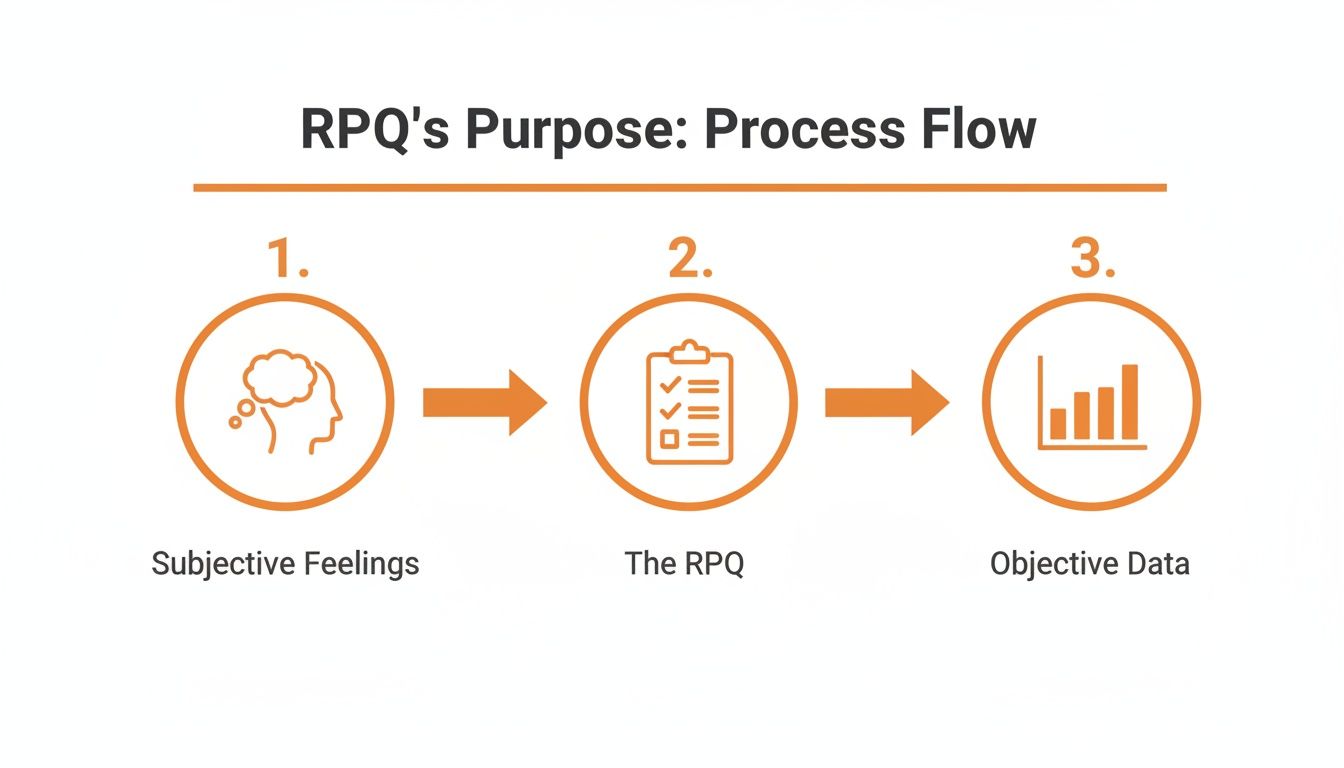
This process is what moves you from just listening to a patient's complaints to building a specific, measurable profile of their recovery.
Getting the Administration Right
The key to getting clean, useful data from the RPQ is making sure the patient knows exactly what you're asking. The questionnaire uses a straightforward 5-point Likert scale, but the context is absolutely critical.
Each symptom is rated based on how it has changed since the injury. This is the most important distinction, as many of these symptoms—like fatigue or headaches—can pop up in anyone's daily life.
The scoring scale is simple:
0: Not experienced at all.
1: No more of a problem than before the injury (this is their personal baseline).
2: A mild problem.
3: A moderate problem.
4: A severe problem.
Actionable Insight: To ensure consistency, always give a brief, standardized instruction before they begin. You could say something like, "For each symptom, I want you to compare how you feel now to how you felt before your injury. A score of 1 means it's the same as it used to be, while a 2, 3, or 4 means it has become a mild, moderate, or severe problem for you since the accident."
This one simple instruction prevents a world of confusion and drastically improves the quality of the data you collect. For more in-depth guidance on patient assessments, you might find our guide on MoCA assessment instructions helpful.
The Two Ways to Score the RPQ
Once the form is filled out, you've got two main ways to calculate the scores. Each method gives you a slightly different lens through which to view your patient's condition.
1. The Total Severity Score (RPQ-16)
This is the most common and direct approach. You just add up the scores for all 16 items. The final number, which can range from 0 to 64, gives you a single, powerful measure of the patient’s overall symptom burden.
A higher total score signals a greater severity of post-concussion symptoms. This single number is incredibly useful for tracking progress. Seeing that score drop across weekly or monthly assessments is a strong, objective sign that your patient is on the right track.
2. The Subscale Scores (RPQ-3 and RPQ-13)
If you want to dig a bit deeper, you can separate the items into two distinct clusters. This is a great way to pinpoint whether a patient's main struggles are physical or lean more toward the cognitive-emotional side.
RPQ-3 (Physical Symptoms): This score is the sum of just the first three items—headaches, dizziness, and nausea/vomiting. The score ranges from 0 to 12 and gives you a snapshot of those early, somatic symptoms.
RPQ-13 (Cognitive-Emotional Symptoms): This is the total of the remaining 13 items, covering everything from forgetfulness and irritability to sleep disturbance and fatigue. The score ranges from 0 to 52 and shines a light on the cognitive, emotional, and behavioural fallout from the injury.
Breaking the scores down like this helps you get specific with your treatment plan. For example, a patient with a high RPQ-3 score might need interventions focused on vestibular therapy or pain management. On the other hand, someone with a high RPQ-13 score might benefit more from cognitive rehabilitation or psychological support.
A Quick Reference Guide to the 16 RPQ Items and Scoring
To help put this all into practice, here's a handy table that breaks down all 16 symptoms covered in the RPQ. You can use it as a quick reference when reviewing a patient's questionnaire.
Symptom Item | Description of Symptom | Scoring Scale (0-4) |
|---|---|---|
1. Headaches | Experiencing head pain | 0-4 |
2. Dizziness | Feeling lightheaded or unsteady | 0-4 |
3. Nausea and/or vomiting | Feeling sick to the stomach | 0-4 |
4. Noise sensitivity | Bothered by loud noises | 0-4 |
5. Sleep disturbance | Trouble falling or staying asleep | 0-4 |
6. Fatigue | Feeling tired, lacking energy | 0-4 |
7. Being irritable | Feeling easily annoyed or angered | 0-4 |
8. Feeling depressed | Feeling sad or low in mood | 0-4 |
9. Feeling frustrated | Getting easily frustrated | 0-4 |
10. Forgetfulness | Difficulty remembering things | 0-4 |
11. Poor concentration | Trouble focusing attention | 0-4 |
12. Taking longer to think | Slower processing speed | 0-4 |
13. Blurred vision | Vision is not sharp | 0-4 |
14. Light sensitivity | Bothered by bright lights | 0-4 |
15. Double vision | Seeing two images of an object | 0-4 |
16. Restlessness | Feeling unable to stay still | 0-4 |
This table provides a clear overview of the clinical ground the RPQ covers, linking each specific symptom directly to the scoring framework.
Practical Example of Scoring
Let's picture a patient named Sarah. She completes the RPQ two weeks after a minor car accident. She rates her headaches as a '3' (a moderate problem) and gives her dizziness and nausea each a '2' (a mild problem). For the other 13 items, her scores add up to 25.
Here’s how you’d tally her results:
RPQ-3 Score: 3 (headaches) + 2 (dizziness) + 2 (nausea) = 7
RPQ-13 Score: 25
Total Severity Score (RPQ-16): 7 + 25 = 32
This initial score of 32 gives you a solid baseline to work from. More importantly, the subscale scores tell you that while her physical symptoms are definitely there, her cognitive-emotional symptoms are the bigger piece of the puzzle right now. This is a crucial insight that lets you focus your care plan where it's needed most from day one—perhaps by prioritizing cognitive pacing strategies and mental health support over purely physical therapies.
Turning RPQ Scores Into Clinical Insights
A raw score from the Rivermead Post Concussion Symptoms Questionnaire is, on its own, just a number. Its true power comes alive in your hands, during clinical interpretation, where that data gets woven into a clear story about your patient’s recovery. This is where you move past the numbers and start making the informed decisions that truly shape a care plan.
The total score gives you a quick snapshot of the patient's overall symptom burden. A low score might signal mild symptoms that are resolving well, while a higher score points toward more significant challenges. But real insight comes from context—a score means very little without considering the patient's history, how long it's been since the injury, and your other clinical findings.

From Numbers to a Narrative
Interpreting the RPQ is really about looking for patterns. The way the scores are distributed across the 16 items can tell you which symptom clusters are most problematic for a patient. This helps you zero in on specific areas that need attention and start tailoring your interventions.
Practical Example: Consider two different patients who both have a total RPQ score of 30:
Patient A: Scores highly on physical items like headaches (4), dizziness (4), and light sensitivity (3). Their cognitive scores for forgetfulness and concentration are much lower (1s and 2s). This profile paints a picture of a recovery that’s primarily hampered by somatic and sensory issues.
Patient B: Reports low scores for physical symptoms but high scores on cognitive items like poor concentration (4), taking longer to think (4), and forgetfulness (3). This patient’s profile suggests that cognitive and emotional difficulties are the real drivers of their symptom load.
Even with identical total scores, their recovery needs are worlds apart. Actionable Insight: For Patient A, you might prioritize vestibular therapy or headache medication. For Patient B, you would likely focus on cognitive rehabilitation strategies and support. This is how the RPQ guides you toward more personalized and effective care. You can find more on building a robust strategy in our guide to complete concussion management.
Charting the Recovery Trendline
The RPQ is most powerful when you use it for serial assessments over time. By administering the questionnaire at regular intervals—say, weekly in the acute phase, then bi-weekly or monthly—you can create a recovery trendline. This visual map of their progress is an invaluable clinical tool.
A recovery trendline does more than just track symptoms; it visualizes the patient's healing journey. A downward slope is a powerful, objective confirmation of progress, while a plateau or spike can be an early warning sign that an intervention needs to be adjusted.
For instance, if a patient’s scores are steadily dropping but then suddenly jump up, it forces you to ask important questions. Did they return to work too soon? Are they dealing with new stressors at home? This data-driven approach lets you make proactive adjustments to their treatment plan instead of waiting for a major setback to happen.
Understanding Normative Data
To add another layer of context, it helps to know what scores look like in the bigger picture. A significant Canadian study at the Hull-Ellis Concussion and Research Clinic in Toronto, for example, tracked adults after a concussion. They found a mean total score of 21.0 across over a thousand assessments, with patients reporting an average of 10.2 symptoms. Data like this helps you benchmark your patient's score against a larger cohort, giving your clinical judgment a stronger foundation. You can discover more from the Workplace Safety and Insurance Board.
Ultimately, turning RPQ scores into insights is an art that's backed by science. It requires blending the quantitative data from the questionnaire with your qualitative clinical expertise. By focusing on symptom patterns, tracking trends over time, and putting the scores into context, you can use the Rivermead Post Concussion Symptoms Questionnaire to its full potential and create a clearer path to recovery for every single patient.
Pairing Subjective Reports with Objective Cognitive Data
The Rivermead Post Concussion Symptoms Questionnaire gives you a powerful window into a patient’s subjective world. It’s the story of their recovery, told in their own words. It tells you what they feel.
But to get the full, 360-degree picture of their brain health, you need to pair that story with hard data showing how their brain is actually performing.
This is where the magic really happens—in the synergy between what a patient reports and what we can objectively measure. Think of yourself as a detective. The RPQ is the crucial witness testimony; it’s the personal account of what’s going on. Objective cognitive assessments? That’s your forensic evidence. It’s the hard, measurable data that either confirms, quantifies, or adds critical context to that testimony.
Validating Patient Reports with Hard Data
Let’s walk through a common scenario. A patient fills out the RPQ and circles a '4' (severe problem) for "poor concentration." This tells you concentration is a major struggle for them, but it doesn't really tell you the whole story. Just how severe is this deficit compared to a healthy baseline? Is it an issue with their processing speed? Their executive function? Or both?
This is exactly where objective measurement becomes indispensable.
An objective cognitive assessment can precisely measure key domains like:
Sustained Attention: How long can they genuinely stay on task before their performance starts to drop off?
Processing Speed: How quickly can their brain absorb and react to new information?
Executive Function: What's their real capacity for planning, solving problems, and juggling competing demands?
By testing these functions directly, you can validate the patient's subjective complaint of "poor concentration." More importantly, you can quantify the specific nature of the problem. This data-driven clarity cuts through diagnostic uncertainty and lets you build a highly targeted and effective therapy plan from day one.
The Power of a Combined Approach
When you weave together subjective and objective data, you create a clinical picture that is far more robust and reliable. This doesn't just sharpen your diagnostic accuracy; it deepens your entire understanding of the patient's condition.
For example, a key Canadian study on mild traumatic brain injury (mTBI) used the RPQ to track how early symptoms could predict long-term outcomes. The researchers found that higher initial RPQ scores were significantly linked to a poorer recovery six months down the line. This really underscores the questionnaire's predictive value.
The RPQ's subjective data is clearly vital. But when you complement it with objective metrics, you’re building your care plan on an even stronger foundation. To get this objective data, clinicians often turn to tools that can measure specific cognitive functions. For instance, the TOVA test, an objective cognitive assessment, can provide valuable data on attention and impulsivity, both of which are crucial for understanding post-concussion challenges.
A Practical Example of Integration
Imagine a patient, David, who is six weeks post-concussion.
RPQ Report (Subjective): David scores high on fatigue, frustration, and "taking longer to think." His total score is concerning, but those specific cognitive complaints are what really jump out.
Objective Assessment (Objective): You run a digital cognitive assessment. The results are clear: his processing speed is in the 15th percentile for his age, and his working memory is in the 22nd percentile.
Suddenly, you have the complete picture. David doesn't just feel slow; his brain is measurably processing information at a much slower rate. His frustration isn't just an emotional symptom; it’s likely a direct consequence of his brain struggling to keep up with the cognitive demands of his day. Actionable Insight: This allows you to zero in on rehabilitation that targets processing speed while providing him with practical strategies (like using reminders or breaking down tasks) to compensate for his memory deficits.
The visual breakdown of cognitive performance across different domains makes it easy to spot strengths and weaknesses at a glance, perfectly complementing the symptom severity scores from the RPQ.
By combining the 'what' from the Rivermead Post Concussion Symptoms Questionnaire with the 'how' and 'how much' from objective tests, you create a powerful diagnostic and therapeutic loop. You can track both symptom perception and functional performance, ensuring your treatment plan is addressing the patient's entire experience.
Platforms like Orange Neurosciences are designed to deliver these critical objective metrics efficiently. Our AI-powered tools can generate a detailed cognitive profile in under 30 minutes, giving you immediate data that fits seamlessly with the insights you've already gathered from the RPQ. This fusion of subjective and objective assessment is the cornerstone of modern, evidence-based concussion care.
To see how this works, learn more about our advanced cognitive assessments and start building a more complete picture of your patients' brain health today.
Common Pitfalls and Considerations When Using the RPQ
While the Rivermead Post Concussion Symptoms Questionnaire is a powerful tool in any clinician's toolkit, its true value comes from using it wisely. Like any self-report measure, it comes with a few quirks and limitations that we need to keep in mind to avoid misinterpreting the results and to make sure the data we collect actually helps our patients.
First and foremost, the RPQ is subjective. That’s not a flaw, just a fact. A patient's score can be coloured by their mood that day, how motivated they are, or even how well they can actually remember what they felt like before the injury. It’s a reality of patient-reported outcomes that calls for a healthy dose of clinical judgment.
The Non-Specificity of Symptoms
One of the biggest traps is forgetting how non-specific many of the symptoms on the list are. Things like fatigue, irritability, and trouble concentrating aren't exclusive to concussions. Not by a long shot. They can pop up because of depression, anxiety, chronic pain, or just the everyday stress of modern life.
This overlap is exactly why a high RPQ score isn't a diagnosis on its own. Think of it as a signal flare, not the final word.
The RPQ tells you what symptoms are present and how severe the patient feels they are, but it doesn't tell you why. That’s where good clinical work comes in—a thorough interview to connect the dots back to the injury and rule out other culprits.
It might surprise you how common many of these symptoms are in the general population. For example, a study of healthy adults in British Columbia found that 57.3% reported fatigue and 24.1% dealt with noise sensitivity in the last two weeks, all without any head injury. This is a powerful reminder of why we need to compare a patient's score to their own pre-injury baseline, not to some ideal score of zero. You can dig into these community reference values in a Canadian context to see just how common these symptoms are.
Context Is King
Another piece of the puzzle is the patient's own context—their age, pre-existing conditions, and life situation. You can't use the RPQ in a vacuum. It was designed for adults, so while it can be adapted for older teens, you might need to explain some of the language. For young kids, it’s generally not the first tool you’d reach for.
Let's walk through a real-world scenario:
The Patient: A 35-year-old with a known history of generalized anxiety disorder gets a mild concussion.
The RPQ Results: Two weeks later, they score high on restlessness, irritability, and poor sleep.
The Pitfall: It’s easy to chalk all of this up to the concussion. But if you do that, you miss the fact that their pre-existing anxiety can cause the exact same symptoms.
Actionable Insight: The clinician sits down with the patient and talks about their anxiety history. They ask questions to help the patient tease apart their baseline anxiety from what’s new or worse since the injury. This simple conversation prevents an inflated score from sending the treatment plan in the wrong direction.
The point here isn't to knock the Rivermead Post Concussion Symptoms Questionnaire. It’s about using it skillfully, as one important piece of a bigger clinical picture. When you back up these subjective reports with objective data, you get the validation and context you need to build a truly accurate picture of what’s going on.
For a clearer path to recovery, it's essential to combine these insights with objective metrics. Discover how Orange Neurosciences can provide the data you need to validate patient reports by scheduling a personalized demo with our team today.
Frequently Asked Questions About the RPQ
Even after getting a handle on the basics, clinicians and researchers often have questions about putting the Rivermead Post Concussion Symptoms Questionnaire to work in the real world. Let's tackle some of the most common ones to help you start using the RPQ with confidence.
How Often Should I Administer the RPQ?
The simple answer is: it depends on where the patient is in their recovery. The key isn't a rigid schedule, but consistency. That's how you build a meaningful recovery timeline.
In the acute phase, which is usually the first 2-4 weeks after the injury, a weekly check-in with the RPQ is a great approach. Symptoms can change on a dime during this period, and weekly administrations let you catch those shifts as they happen.
Once you move into later-stage rehab or are dealing with persistent symptoms, a weekly questionnaire can start to feel like a burden. In these situations, switching to every 2-4 weeks is much more practical. It's enough time to see real trends emerge without causing survey fatigue for your patient.
Here's a practical example: A patient is two weeks post-concussion, and their RPQ score has dropped from 35 to 28—great news. But at their three-week check-in, the score suddenly jumps back up to 33. This data point immediately flags a problem. A quick conversation reveals they tried returning to part-time work too soon, allowing you to adjust their recovery plan right away.
Is the RPQ Appropriate for Children and Adolescents?
The original RPQ was built and tested for adults. That said, it's often used effectively with older adolescents, typically those aged 16 and up, as long as there's some guidance.
For younger kids, other tools like the Post-Concussion Symptom Scale (PCSS) are usually a better fit because they were specifically designed for a pediatric population. Younger children can struggle with some of the more abstract concepts on the RPQ, like 'frustration' or 'restlessness,' and interpret them differently than an adult would.
Actionable Insight: If you do decide to use the RPQ with a teen, walk through the questions with them the first time. This ensures they understand what each item is asking, which leads to much more reliable data. For any pediatric evaluation, you'll get the clearest picture by pairing a symptom scale with objective, engaging cognitive assessments.
How Does the RPQ Differ from the SCAT5?
This is a common point of confusion. While both are staples in concussion care, the RPQ and the SCAT5 are designed for different jobs at different moments. Think of them as complementary tools for separate stages of the journey.
SCAT5 (Sport Concussion Assessment Tool): This is your go-to for an acute, on-the-sidelines evaluation right after a suspected injury. Its entire purpose is to help make that crucial "remove from play" decision in the heat of the moment. It has a symptom checklist, but it also includes immediate tests for balance and cognition.
RPQ: This is a much more detailed questionnaire used in a clinical setting for ongoing monitoring. You'll use it to track recovery over weeks or even months, helping to guide return-to-learn and return-to-play decisions long after the initial incident. It’s focused solely on how symptom severity is changing over time.
In short, the SCAT5 is for the immediate aftermath; the RPQ is for the longer haul of recovery. While their scores often correlate, they are absolutely not interchangeable. To get a better sense of the broader assessment landscape, our guide on what is neuropsychological assessment is a great place to start.
Where Can I Find a Copy of the RPQ?
Finding a copy of the Rivermead Post Concussion Symptoms Questionnaire is straightforward. It's widely available for clinical and research use and isn't protected by copyright.
You can usually find a downloadable PDF in a few reliable places:
Academic Databases: A quick search on PubMed or Google Scholar for the original validation studies will often turn up a copy in the paper's appendix.
Clinical Guidelines: Many national and regional health organizations include the RPQ directly within their official concussion management protocols.
Public Health Bodies: Organizations like workers' compensation boards or public health agencies often host PDF versions of the questionnaire as part of their TBI resource packages.
Just be sure you're using the standard 16-item version with the 0-4 scoring scale. Sticking to the official format is crucial for consistency and for making sure your results are comparable to established research and norms.
At Orange Neurosciences, we know that a true understanding of brain health comes from combining what a patient reports with what we can objectively measure. The RPQ tells you the "what"—the symptoms they feel. Our AI-powered platform delivers the "how much" by precisely measuring their cognitive function.
Ready to move beyond guesswork and build data-driven care plans? Visit https://orangeneurosciences.ca to see how our rapid, objective assessments can complement the insights you gain from the Rivermead Post Concussion Symptoms Questionnaire. You can also contact us for a personalized demo to see these tools in action.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation