Comorbidity in ADHD: Essential Guide to Integrated Care & Strategies
Mar 27, 2026

When we talk about Attention-Deficit/Hyperactivity Disorder, it's easy to picture it as a single, isolated condition. But in my experience, both as a clinician and a researcher, that’s rarely the whole story. More often than not, ADHD brings friends to the party—other conditions that exist right alongside it. This is what we call comorbidity.
Put simply, it means someone is navigating the challenges of ADHD plus one or more separate conditions, like anxiety, depression, or a learning disorder, all at the same time. Understanding this overlap isn't just an academic detail; it's the key to unlocking effective diagnosis and treatment. In this guide, we'll give you practical examples and actionable insights to help you navigate this complex landscape. For more resources, you can always visit our website.
Why ADHD Rarely Travels Alone

One of the first things any new clinician or concerned parent needs to grasp is that ADHD almost never shows up by itself. Think of it less like a single tree in a field and more like a tree in a dense forest, where the root systems are all tangled together.
The brain is an interconnected system. The same neurological pathways and executive functions that are impacted by ADHD also play a role in regulating mood, behaviour, and learning. A struggle in one area can easily cause a ripple effect, creating symptoms that look a lot like another disorder.
Here's a practical example: a child who can’t focus in class might have ADHD. Or, they could be so consumed by anxiety that their working memory is overloaded, making focus impossible. Or, it could be both. This is the clinical puzzle we face every day, and it’s why just looking at surface-level symptoms isn't enough. The actionable insight here is to always ask why a behavior is happening before jumping to conclusions.
The Numbers Tell the Story
Just how common is this overlap? The statistics are staggering and paint a very clear picture. It's not the exception—it's the rule.
The table below, based on recent national health survey data, shows just how prevalent co-occurring conditions are for children with ADHD.
ADHD Comorbidity Prevalence at a Glance
Statistic | Percentage / Figure |
|---|---|
U.S. Children (3-17) Diagnosed with ADHD | 11.4% |
Children with Current ADHD and a Co-occurring Disorder | 77.9% |
- With a Behavioural/Conduct Problem | 47.9% |
- With an Anxiety Disorder | 39.1% |
- With Depression | 18.9% |
These numbers drive home a critical, actionable point: for the vast majority of kids, an ADHD diagnosis is just the starting point. We aren’t just treating ADHD; we are managing a complex and interconnected profile of needs. This is a fundamental shift in perspective that is crucial for effective care, and it often involves understanding the connection between autism, ADHD, and mental health as well.
Thinking in terms of comorbidity forces us to move beyond a single label. It’s about seeing the whole person—their unique cognitive and emotional landscape—so we can create interventions that actually work for them.
Moving Beyond a Single Label
When we start looking for comorbidities, we stop settling for easy answers. It pushes us as clinicians and caregivers to dig deeper during an evaluation, moving past the obvious symptoms to uncover the full picture of what a person is experiencing.
Seeing that full picture is everything. It allows us to build a support system that addresses every facet of an individual's challenges, not just the most visible ones. This integrated approach is what leads to real, lasting progress. In this guide, we’ll explore how to spot these co-occurring conditions, understand where they come from, and design treatment plans that address the whole person. To stay updated with more insights like these, consider visiting our website for more guides and resources.
Identifying Common Co-Occurring Conditions
So, you’ve come to understand that ADHD rarely travels alone. That’s a huge first step. The next, and arguably more critical one, is learning to spot the common companions it keeps. Pinpointing comorbidity in ADHD isn’t about memorizing a textbook; it’s about recognizing the subtle (and sometimes not-so-subtle) ways these other conditions weave themselves into daily life.
Think of yourself as a detective. Your main investigation might be ADHD, but a good detective knows to look for clues that point to a bigger, interconnected story. These clues often hide in plain sight, easily mistaken for behaviours you’d just chalk up to ADHD.
Anxiety and Mood Disorders
Anxiety is, by far, one of the most frequent visitors. While the ADHD brain can feel overwhelmed by the chaos of the outside world, anxiety creates a storm on the inside. Telling them apart can be tricky because they often look the same from the outside.
Here’s a practical example: A child with ADHD might not start their homework because their executive functions are making it a nightmare to simply begin the task. But a child with both ADHD and anxiety might be staring at the same blank page, completely frozen by a deep-seated fear of making a mistake. The behaviour is identical—the homework isn't getting done—but the engine driving it is entirely different. An actionable insight for parents is to ask about their child's feelings ("What's on your mind when you look at the homework?") instead of just focusing on the behavior.
Mood disorders like depression throw another wrench into the diagnostic works. The exhaustion and total lack of motivation you see in depression can look an awful lot like the task-initiation struggles that are a hallmark of ADHD.
One of the best ways to tell the difference is to look at how widespread the feeling is. Is the lack of motivation specific to certain tasks and situations? That often points to ADHD. Or has a persistent shadow of sadness and a loss of joy (anhedonia) fallen over nearly every part of life? That's more typical of depression.
Disruptive Behaviour and Learning Disorders
It's also incredibly common to see ADHD alongside disruptive behaviour disorders like Oppositional Defiant Disorder (ODD) and Conduct Disorder (CD), especially in kids and teens. It's all too easy to label a teenager as simply "defiant," when in reality, their behaviour is a desperate reaction to cognitive struggles they can't articulate.
Imagine a teen who constantly refuses to follow a parent's multi-step instructions. Is it pure defiance? Or could it be that their ADHD-related working memory deficits make it literally impossible to hold onto all the steps at once? Feeling overwhelmed and frustrated, they lash out or just shut down entirely. What looks like ODD is actually a coping mechanism gone wrong. The actionable takeaway is to simplify instructions and check for understanding, rather than escalating the confrontation.
The research backs this up. A massive analysis of almost six million patients found that 19.72% of individuals with ODD also had ADHD. The link with Conduct Disorder was even stronger, at 20.87%. The connections run deep.
Autism Spectrum Disorder and Sleep Issues
The overlap between co-occurring Autism and ADHD (AuDHD) presents a particularly unique and complex picture. Since both are neurodevelopmental conditions, they can create a confusing and often conflicting internal experience.
Routine vs. Novelty: An individual might desperately crave the predictable, soothing structure that calms their autistic traits, while at the same time feeling the intense boredom and pull for novelty driven by their ADHD.
Social Interaction: They might genuinely desire social connection (an ADHD trait) but feel completely overwhelmed and drained by the effort of decoding social cues (an autistic trait).
This constant internal tug-of-war is a classic sign of AuDHD and demands a truly nuanced approach from clinicians and caregivers. If you're trying to better understand the diagnostic process, our guide on how an autism assessment is conducted is a great place to start.
Finally, we have to talk about sleep. Sleep disorders are practically a given in the ADHD population. The restless, "always-on" ADHD brain often refuses to power down at night. This leads to a cascade of problems: trouble falling asleep, staying asleep, and waking up feeling anything but refreshed. Of course, this chronic sleep deprivation just pours fuel on the fire, making symptoms like inattention and emotional dysregulation even worse the next day. It’s a vicious cycle.
Recognizing these common co-occurring conditions is the bedrock of effective support. When we look beyond the primary diagnosis, we can finally start to build a plan that addresses the whole person—not just one piece of the puzzle.
Unpacking the Roots of Comorbidity
After seeing which conditions so often show up with ADHD, the natural question is why. Is it simply a case of bad luck, or are there deeper, more fundamental connections at work? The answer, as it turns out, is a rich mix of genetics, brain wiring, and lived experience.
Understanding these drivers is what allows us to see comorbidity in ADHD not as a random list of separate problems, but as a deeply interconnected web. It’s not just about having two conditions at once; it’s about how they are wired together beneath the surface. This understanding offers an actionable insight: treatment must be integrated, not siloed.
Shared Genetic Signatures
First, let's look at our genes. A growing body of research shows that ADHD and many of its common companions, like anxiety and depression, often share the same underlying genetic markers. It’s important to understand that these aren't single "genes for ADHD" or "genes for anxiety." Instead, think of them as complex combinations of genetic variations that create a predisposition for certain neurodevelopmental traits.
Here's a practical example: Imagine your DNA is a massive, intricate blueprint for building a city. A certain set of instructions might lead to a transportation system (your brain’s neural pathways) that's incredibly efficient in some ways but also prone to major traffic jams under stress. This could show up as both the executive function struggles of ADHD and the overwhelming feelings of anxiety. You inherit the blueprint, not the traffic jam itself.
An Israel-wide population study drove this point home, finding that siblings of individuals with ADHD are not only five and a half times more likely to have ADHD themselves, but also 40% more likely to have anxiety or personality disorders. This points directly to a shared familial and genetic vulnerability that doesn’t stop at the border of a single diagnosis.
Overlapping Brain Wiring
Beyond genetics, the brain's own structure and function play a pivotal role. ADHD is strongly linked to differences in the prefrontal cortex—the brain's "air traffic controller" that manages our executive functions like attention, emotional regulation, and impulse control.
Think of it like a city's power grid. If the main control centre (the prefrontal cortex) has some faulty wiring, it won't just cause the lights to flicker in one building (attention). It might also cause power surges in the emotional regulation district and brownouts in the planning and organization sector. The very same core neurological issue can produce a wide range of symptoms that we end up labelling as different disorders.
This concept of shared neurobiology is a game-changer. It explains why a child struggling with emotional outbursts (often seen in ODD) might also have a terrible time trying to plan a school project (an ADHD-related executive function deficit). Both challenges can spring from the exact same underlying difficulties in the prefrontal cortex.
The Impact of Lived Experience
Finally, we absolutely cannot ignore psychosocial factors. Living with the daily friction of untreated ADHD is incredibly stressful. The constant cycle of struggling to meet expectations, facing social rejection, and feeling like you’re always two steps behind can take a heavy toll on a person's mental health.
For instance, a child who is constantly being corrected for interrupting in class isn't just learning to be quiet. They might be internalizing the painful message that they are "bad," "annoying," or "broken." Over time, this chronic stress and negative self-perception can directly trigger or worsen secondary conditions like anxiety and depression. An actionable insight for teachers and parents is to focus on scaffolding success and praising effort, which can build resilience and counter these negative narratives.
A Swedish study found that mothers with ADHD had a five times higher risk of postpartum depression, a stark example of how the inherent challenges of ADHD can amplify vulnerability during stressful life events. Understanding this cascade effect is crucial. It’s how we move from just treating symptoms to designing interventions that support the whole person. To get a clearer picture of how these factors are evaluated, you can learn more about what a neuropsychological assessment involves and how it helps map these complex connections.
Untangling the Knot: Differentiating ADHD from Its Look-Alikes
One of the trickiest parts of managing comorbidity in ADHD is that the symptoms just don't stay in their neat little boxes. Think about a child who can’t focus in class. That’s the classic sign for ADHD, right? But is it truly an issue with attention, or could it be an anxiety disorder that’s eating up all their mental energy, making it impossible to concentrate? This is the exact spot where a treatment plan can go sideways before it even gets started.
This symptom overlap often creates a kind of "masking" effect, where the louder symptoms of one condition completely drown out another. A practical example is the non-stop fidgeting of hyperactivity, which can easily hide the quiet, internal storm of anxiety. A clinician might see a child who can't sit still and jump straight to an ADHD diagnosis, completely missing the constant, paralyzing worry that’s actually fuelling all that movement.
To untangle this, we have to look deeper than a simple screening. It’s all about asking the right questions to get to the root of the behaviour, not just what's on the surface.
From Symptom to Source
The real breakthrough happens when we shift our focus from what the symptom is to why it’s happening. A report of "trouble concentrating" isn't a diagnosis; it's a clue.
Let’s put this into a real-world context. Imagine two students who are both struggling to finish their math homework.
Student A (ADHD-driven): He starts the worksheet, but then a bird lands on the windowsill. He gets distracted, forgets the instructions, and starts doodling in the margins. The real problem here is a breakdown in sustained attention and working memory.
Student B (Anxiety-driven): She just stares at the blank page, completely overwhelmed by the fear of getting the answers wrong and being seen as "stupid." Her issue isn't attention; it's performance anxiety that’s put a freeze on her ability to think.
The result is the same—an incomplete assignment—but the cause is worlds apart. An actionable insight for educators is to observe how a student fails, not just that they failed. This observation is key to providing the right support.
A Clearer Picture with Objective Data
This is where relying only on what you see or what a parent tells you can lead you down the wrong path. Adding an objective cognitive profile, like the one from Orange Neurosciences, gives you a critical piece of the puzzle. It takes you beyond what a patient says is happening and measures what their brain is actually doing.
To help clinicians distinguish between these overlapping conditions, this table highlights some key differences in how common symptoms might present.
Differentiating ADHD from Common Comorbidities
Symptom | Presentation in ADHD | Presentation in Anxiety | Presentation in Depression |
|---|---|---|---|
Inattention | Trouble sustaining focus, easily distracted by external stimuli, makes careless mistakes. Often jumps from task to task. | Difficulty concentrating because of intrusive worries or fears. Mind goes blank due to performance anxiety. | Poor concentration due to low energy, lack of interest (anhedonia), and slowed thinking. |
Restlessness/Fidgeting | A persistent feeling of inner restlessness, constant physical movement, inability to stay seated. Often seems "driven by a motor." | Physical tension, fidgeting, or pacing driven by worry and nervousness. May be situational (e.g., before a test). | Psychomotor agitation can occur, but it's often paired with low mood. Can also present as psychomotor retardation (slowed movement). |
Task Avoidance | Avoids tasks that require sustained mental effort (e.g., homework) because they are perceived as boring or difficult. | Avoids tasks or social situations due to fear of failure, judgment, or negative outcomes. Perfectionism can lead to procrastination. | Avoids tasks due to overwhelming fatigue, feelings of hopelessness, or a sense of worthlessness. Lacks the motivation to start. |
This table is a starting point, but a comprehensive assessment is always needed to make a definitive diagnosis.
A parent might say their child has "brain fog." Objective data can tell us if that fog is caused by slow processing speed (common in ADHD), a breakdown in attentional control, or a working memory system that’s overloaded by the constant hum of anxiety. That kind of clarity is a game-changer.
This complex overlap isn't random. It often stems from shared biological roots and environmental triggers, as this chart helps to explain.
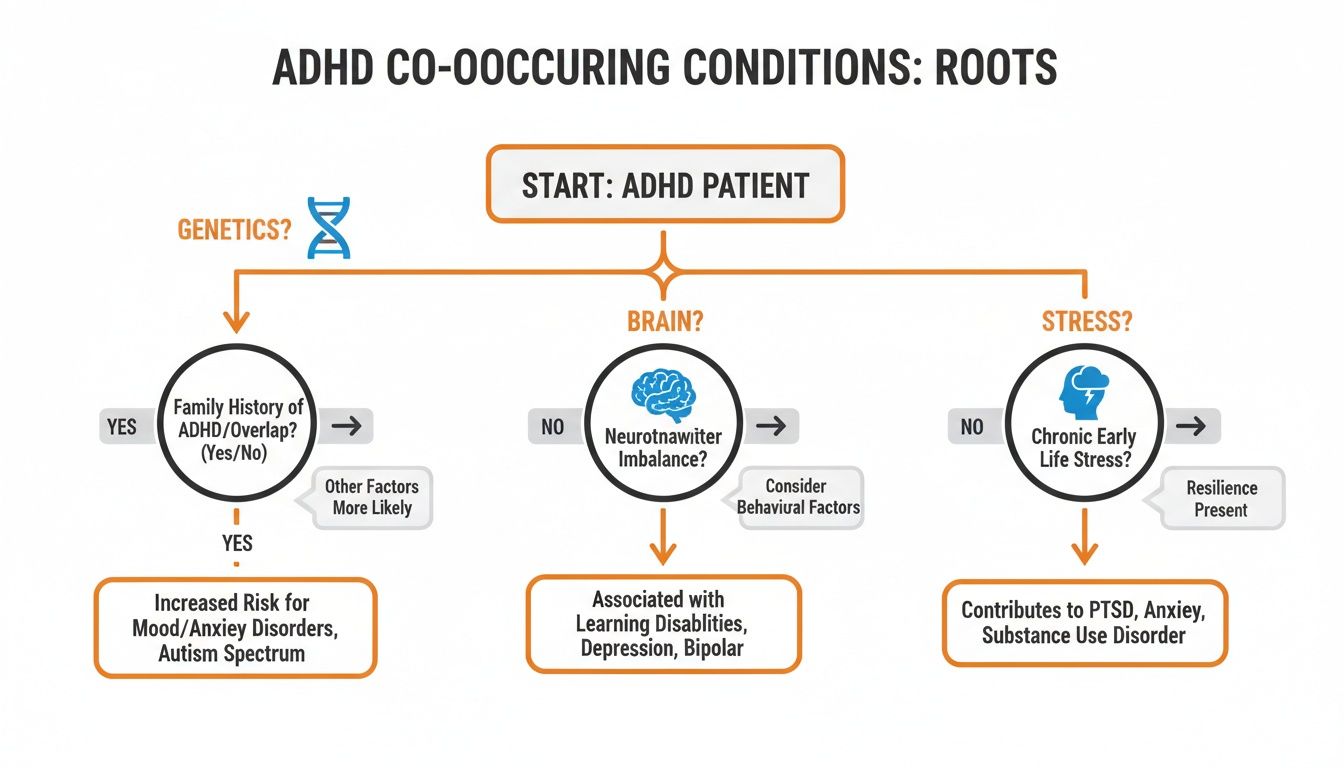
What this shows us is that a person's final diagnosis is often the result of a delicate dance between their genes, their unique brain wiring, and the stressors they've faced in life.
By adding objective data to the mix, we can stop guessing. We can see if a person’s cognitive profile fits the typical patterns of ADHD, or if their cognitive struggles look more like a side effect of anxiety or depression. This allows for a diagnosis that truly reflects what’s going on inside their brain, opening the door to treatment that is targeted and genuinely effective. To learn more about this process, our guide to a complete mental health assessment goes into greater detail, and our website offers further resources.
Building an Integrated Treatment Plan That Works

Getting the right diagnosis is a huge step, but it’s really just the starting line. When you’re dealing with comorbid ADHD, you can't just treat one condition and hope the others fall into line. We need a unified strategy that looks at the whole person, not just a list of symptoms.
Here's a practical example: it’s like walking into a house renovation where the wiring is faulty (that's your ADHD) and the roof is leaking (let's call that anxiety). If you only fix the wiring but ignore the water damage happening every time it rains, you're setting yourself up for a much bigger problem down the road. A smart plan has to tackle both at the same time, understanding how one problem makes the other worse.
This isn't just a theoretical issue; the complexity we're seeing in clinics is on the rise. A decade-long study from Kaiser Permanente Northern California, for instance, saw adult ADHD diagnoses double between 2007 and 2016. What was driving that surge? In large part, it was the presence of other psychiatric conditions. You can discover more about this trend and its implications for care on the Kaiser Permanente research site.
The Core of an Integrated Plan
An integrated, or multi-modal, plan isn’t about throwing a bunch of different therapies at the wall to see what sticks. It's about weaving them together into a coherent safety net that supports the individual everywhere—at home, in the classroom, and during therapy. Every piece of the plan has to talk to the others.
Typically, this rests on three pillars working in concert:
Pharmacotherapy: This is a delicate balancing act. For someone with both ADHD and anxiety, a clinician won't just prescribe a standard stimulant. They might start with a non-stimulant medication first or choose a specific stimulant known to have a lower risk of making anxiety worse. It requires careful selection and constant communication.
Psychotherapy: This is where we build skills. Cognitive Behavioural Therapy (CBT) is a workhorse here because it’s so adaptable. The same framework can be used to help someone manage the executive functioning deficits of ADHD and challenge the negative thought spirals that come with depression or anxiety.
Behavioural Strategies: This pillar is all about the real world. It’s the practical, day-to-day support, like creating predictable routines at home, getting the right accommodations at school, or coaching parents on how to respond to challenging behaviour in a way that de-escalates conflict instead of fueling it.
Making It Personal with Targeted Interventions
The real magic happens when we move beyond a general approach and get personal, using objective data to guide us. When a detailed assessment pinpoints a specific cognitive weakness that's fueling symptoms across different conditions, we can aim our interventions with incredible precision. It’s so much more effective than treating each diagnosis in its own silo.
Here's an actionable insight in practice: Imagine an assessment with a tool like ReadON shows a significant working memory deficit. That one cognitive snag could be the engine behind a child's ADHD-related inattention and their struggles with reading comprehension. Instead of splitting our efforts between reading tutoring and separate behavioural therapy for focus, we can build a plan that includes targeted cognitive training to strengthen that core working memory skill.
This gives us a massive advantage. As the child's working memory improves, you’ll almost certainly see a ripple effect. Their ability to follow multi-step instructions gets better, and their reading flows more easily. To dig deeper, you can check out our guide on the crucial link between ADHD and working memory.
By building a plan that’s truly integrated, we finally get to stop playing that frustrating game of symptom "whack-a-mole." Instead, we start getting to the root of the problem, giving individuals the tools they need to manage their unique brain and truly thrive. Ready to learn more about how we can help? Visit our website today.
Where to Go from Here: Managing Comorbid ADHD in Practice
Knowing the theory behind comorbidity in ADHD is one thing, but confidently handling these overlapping conditions in the real world is where it truly counts. Let's move from the 'what' to the 'how,' with clear, actionable steps for both clinicians and caregivers.
The first place to start is your intake process. Just asking, "Does your child have trouble focusing?" is far too wide a net. We need to dig deeper and understand the why behind the behaviours we're seeing.
Asking Better Screening Questions
It’s time to weave in specific questions designed to gently uncover hidden anxiety, depression, or other issues that might be travelling with ADHD. These prompts help you start untangling the roots of a particular struggle.
Here is a practical, actionable list of questions you can adapt for your conversations:
"How often does the fear of making a mistake stop you from even starting something?" (This is a great way to tease apart anxiety-based avoidance from classic ADHD procrastination.)
"When you feel restless, is it more like your body just needs to move, or is it an inner feeling of being tense and on edge?" (This can help distinguish physical hyperactivity from the internal buzz of anxiety.)
"Do you find yourself always looking for new and exciting things to do, or do you feel much better with familiar routines and find change upsetting?" (This can give you a clue about a potential overlap with ASD.)
Asking these kinds of nuanced questions paints a much richer picture right from the start. They help you see if you're looking at a straightforward ADHD presentation or something more complex.
When a patient’s answers hint at a complicated picture, or when the first-line ADHD strategies just aren't working as you'd expect, that’s your signal. It's a clear sign that it's time to dig deeper with a more comprehensive evaluation. This is where objective data becomes your most trusted guide.
Using Objective Data to Guide and Track Progress
A full neuropsychological evaluation, informed by objective cognitive data, takes the guesswork out of the equation. Tools from Orange Neurosciences can establish a precise cognitive baseline, measuring core skills like working memory, processing speed, and attentional control.
This data isn't just for getting the diagnosis right. It becomes a powerful roadmap for tracking progress.
You can actually measure how your interventions are affecting specific cognitive functions. This lets you prove what’s working, fine-tune your strategies based on hard data, and show real, tangible improvement to patients and their families.
Managing complex cases of comorbidity in ADHD doesn't have to feel like navigating in the dark. With the right tools and a clear, systematic approach, you can provide targeted, effective care that addresses the whole person.
Ready to see how objective cognitive assessment can become your greatest asset in complex cases? Visit our website to learn more about our platform or book a demo.
Frequently Asked Questions
When we talk about ADHD, the conversation rarely stops there. It's a complex condition, and many of the clinicians and caregivers I speak with are trying to make sense of the overlapping symptoms and diagnoses that so often come with it. Let's tackle some of the most common questions with practical answers.
Which Comorbidity Is Most Common With ADHD in Children Versus Adults?
The co-occurring conditions we see most often really do change as a person grows. With children, the most visible challenges are often behavioural. We see Oppositional Defiant Disorder (ODD) in almost half of kids with an ADHD diagnosis, making it incredibly common. Anxiety disorders are a very close second.
As children become adults, that picture tends to shift. While defiant behaviours can certainly hang on, the internal struggles often take centre stage. Anxiety and mood disorders, especially depression, become the most frequent partners to adult ADHD. This is also when we start to see substance use disorders appear as a significant concern, often as a way of self-medicating the daily struggles of life with an unmanaged or complex condition.
How Can You Tell if Inattention Is From ADHD or Depression?
This is one of the great diagnostic puzzles we face, and getting it right is critical. The key is to look at the pattern. Inattention from ADHD is a lifelong trait, a core feature of a person's neurodevelopment that shows up consistently across different settings—at school, at home, in relationships, and at work. It's always been there.
Inattention rooted in depression, on the other hand, tends to be episodic. It comes and goes with the person's mood. It's usually wrapped up with other tell-tale signs of depression, like a profound loss of interest in things they once enjoyed (anhedonia), a persistent cloud of sadness, or a deep sense of hopelessness. The inattention is a symptom of the mood, not a standalone trait.
An actionable insight for clinicians: this is exactly where objective cognitive testing can cut through the fog. A cognitive profile might clearly show a primary deficit in working memory—a classic hallmark of ADHD. Or, the data could reveal that the cognitive struggles are more scattered and change depending on the person's reported motivation, which often points to depression as the driving force.
Can Treating ADHD Also Help With Comorbid Conditions?
Yes, very often it does. When we effectively treat the core symptoms of ADHD, it's like a stone tossed into a pond—the positive effects ripple outwards.
Here's a practical example: a person's executive functions improve with the right support, whether that's therapy, medication, or both. Suddenly, they're not failing as much at school or fumbling tasks at work. This simple reduction in daily struggle can powerfully ease the secondary anxiety and depression that grew in the shadow of those constant negative experiences.
But, and this is a big "but," treating ADHD isn't always a magic cure-all. A severe anxiety disorder, major depression, or a substance use disorder are serious conditions in their own right. They demand their own specific, evidence-based treatments. The most powerful approach is always an integrated one—a care plan that addresses every piece of the puzzle at the same time. This is how we build a foundation for genuine, long-term well-being.
Understanding the full cognitive profile is the first step toward building that effective, integrated plan. The AI-powered tools from Orange Neurosciences provide the objective data needed to move beyond guesswork.
Discover how our platform can bring clarity to complex cases by booking a demo today.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation