Montreal Cognitive Assessment vs MMSE: Which Test is Best?
Apr 5, 2026
When you're standing at a clinical crossroads, deciding between the Montreal Cognitive Assessment (MoCA) and the Mini-Mental State Examination (MMSE), the choice boils down to one thing: the clinical question you need answered. The core difference is sensitivity. The MoCA is far better at picking up mild cognitive impairment (MCI), while the MMSE is a faster, blunter instrument often used for tracking decline in more established dementia.
MoCA vs MMSE: A Clinician's Quick Guide
For any of us on the front lines, choosing between the MoCA and the MMSE is a frequent decision. It’s not about which test is “better” overall, but which is the right tool for this specific patient, right now. While they both look like simple screeners, they were built for different jobs and have very distinct clinical strengths.
The MoCA really shines where the MMSE often stumbles: identifying those subtle, early cognitive deficits. By including more challenging tasks that probe executive function and visuospatial skills, the MoCA is the clear choice for higher-functioning individuals or when your clinical suspicion points toward early-stage changes. These tools are absolutely vital when evaluating patients, especially when a family first raises concerns about the early signs of dementia.
Practical Example: You have a patient with a university education and early Alzheimer’s disease. They score a "normal" 27/30 on the MMSE because it’s too easy for them. That same patient would almost certainly reveal clear deficits on the MoCA—perhaps struggling to draw the clock or naming fewer than 11 animals in the verbal fluency task—triggering an accurate and timely workup. Actionable Insight: If a patient has a high cognitive reserve, default to the MoCA to avoid a false negative.
To help with that quick, in-the-moment decision, here’s a rapid comparison of the two.
Quick Comparison: MoCA vs MMSE
This table breaks down the essential differences to guide your decision-making on the fly.
Feature | Montreal Cognitive Assessment (MoCA) | Mini-Mental State Examination (MMSE) |
|---|---|---|
Primary Use Case | Detecting mild cognitive impairment (MCI) and early dementia. | Screening for moderate-to-severe dementia; tracking progression. |
Sensitivity for MCI | High (90-100%). | Low (18-25%). |
Executive Function | Assessed with tasks like Trail Making B and abstraction. | Not assessed. |
Administration Time | ~10-15 minutes. | ~5-10 minutes. |
Ceiling Effect | Lower; less likely to produce false negatives in educated individuals. | High; often misses deficits in those with higher cognitive reserve. |
Ultimately, choosing the right instrument sets the stage for the entire diagnostic journey that follows.
This screenshot from the official MoCA website perfectly illustrates the domains it covers.
The image confirms what we see in practice: the MoCA gives us a much more thorough look at domains like executive function and visuospatial skills. These are exactly the areas where the first subtle signs of cognitive change often appear. Getting a firm grasp on each tool's scope is the first step, a concept we dive into deeper in our guide on what is cognitive assessment.
Understanding the Origins and Design of Each Test
To really get a handle on the MoCA vs. MMSE debate, you have to go back to their roots. Each test was built to solve a completely different clinical problem, and that history tells you almost everything you need to know about their strengths and weaknesses in practice today.
The Mini-Mental State Examination (MMSE) first appeared back in 1975. Its job was straightforward: give clinicians a quick, practical way to grade the severity of cognitive decline in patients who already had a dementia diagnosis. The test is heavily weighted toward orientation and basic memory recall for a reason.
This focus made it a workhorse for decades, especially for tracking the progression of moderate to severe dementia. The catch? It was designed long before "mild cognitive impairment" (MCI) was a standard clinical term, which is exactly why it tends to fall short in early detection.
The MMSE: A Tool for Grading Known Decline
Because the MMSE was built to quantify significant cognitive loss, its questions are fairly simple. This leads directly to its most notorious problem: the "ceiling effect." You’ve likely seen it in your own practice—patients with high education or cognitive reserve who have genuine, early-stage deficits but still manage to get a perfect or near-perfect score.
Practical Example: Think about a retired accountant whose family is worried about their struggle with managing finances and complex tasks at home. On the MMSE, they might easily score a 28/30 by knowing the date and recalling three simple words. This creates a false negative, giving both you and the family a misleading sense of reassurance.
The MoCA: A Response to the MMSE's Blind Spots
The Montreal Cognitive Assessment (MoCA) was developed in 2005 for one primary reason: to fix the MMSE's blind spots. It was engineered from the ground up to be a more sensitive screener, one that could pick up on the subtle signs of MCI that the MMSE so often misses. It’s why the Montreal Cognitive Assessment vs MMSE choice is such a critical one in any modern memory clinic or primary care setting.
Actionable Insight: The MoCA’s design deliberately includes more complex tasks that probe higher-order cognitive functions. It challenges executive function, visuospatial skills, and more demanding memory recall, making it much harder for a high-functioning person to hide early deficits. If a patient's complaints involve complex, real-world tasks (like finances or planning), the MoCA is the better tool to uncover the underlying cognitive issues.
This simple decision tree illustrates how a patient's presenting concern should guide your choice between the two.
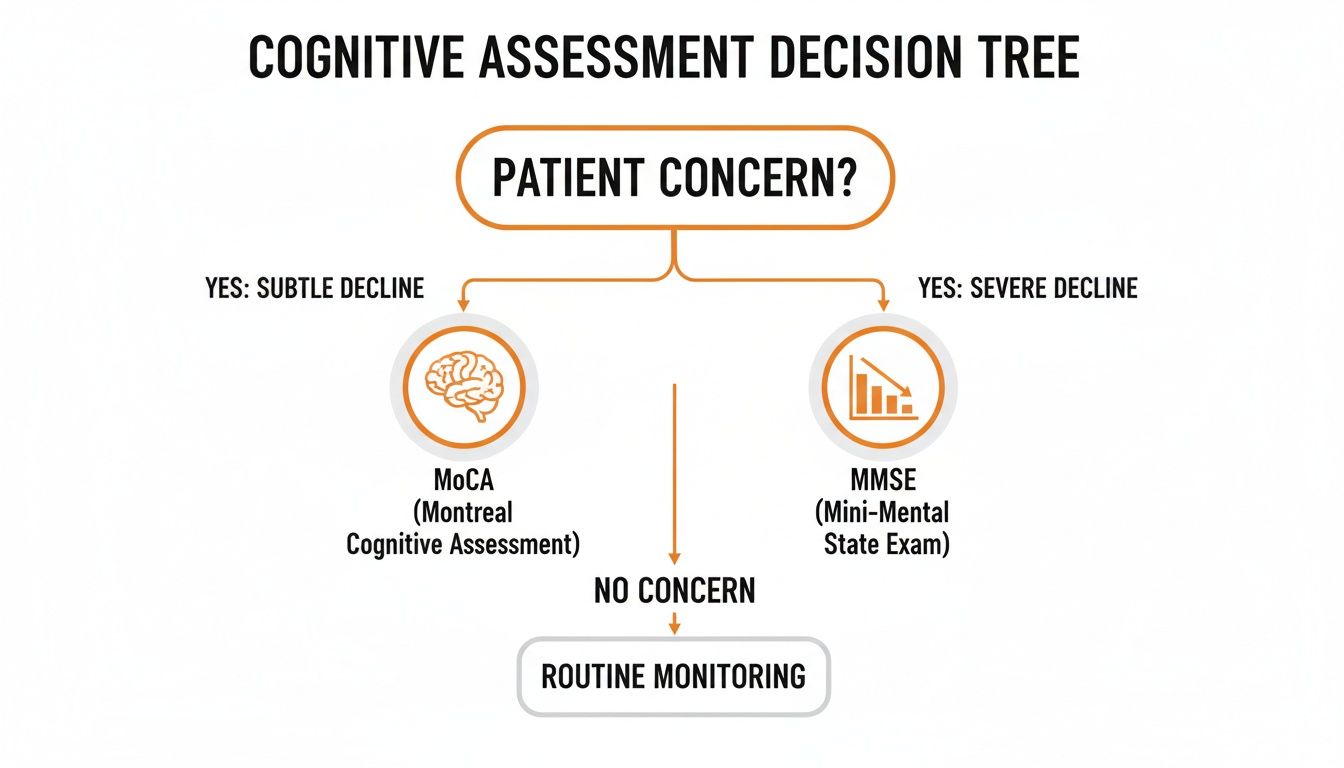
The visual reinforces a simple but powerful rule of thumb. If the concern is subtle change, the MoCA is your go-to. For tracking more advanced, established decline, the MMSE can still be a pragmatic choice.
Let's go back to our retired accountant. On the MoCA, their story would likely be very different. They might struggle with the Trail Making B-style task or find it impossible to draw a three-dimensional cube. Suddenly, the executive and visuospatial issues that the MMSE completely overlooked are brought to light. This ability to unmask hidden deficits is the MoCA's greatest strength.
For a closer look at administration, you can review our guide on the Montreal Cognitive Assessment instructions. Understanding these foundational differences is the first and most crucial step in choosing the right test for the right patient.
Breaking Down the Domains: MoCA vs. MMSE
While it’s tempting to lean on the final score of a MoCA or MMSE for a quick snapshot, the real clinical gold is found by digging deeper. The true value lies in understanding why a patient lost points. A domain-by-domain comparison reveals not just the presence of impairment, but its specific character, which is what really guides your next steps.
It's the difference between knowing a patient is struggling and knowing precisely where they're struggling. This granular detail helps you build a much clearer clinical picture. For instance, a failure on a specific MoCA task can point directly toward frontal lobe deficits—something the MMSE was never really built to catch.

Visuospatial and Executive Function: The MoCA's Clear Edge
The biggest gap between these two tools is the MoCA's robust testing of visuospatial and executive functions. These higher-order cognitive abilities are often the first to show subtle cracks in early neurodegenerative disease.
Practical Example: Let's take the clock drawing task. On the MMSE, a patient might just be asked to copy a clock that's already drawn, a task that tests basic praxis. The MoCA, however, asks them to draw a clock from scratch and set the hands to a specific time, like "10 past 11."
This might seem like a small change, but its clinical impact is massive. A patient who falters on the MoCA's version—maybe by spacing the numbers poorly or misplacing the hands—is showing potential deficits in planning, organization, and abstract thinking. These are core executive functions the MMSE simply doesn't touch.
The MoCA also includes tasks like a simplified Trail Making Test (connecting numbers and letters) and a three-dimensional cube copy.
Trail Making: This tests cognitive flexibility and processing speed. A patient who has trouble here may be struggling to switch between mental sets.
Cube Copy: This directly assesses 3D visuospatial skills. An inability to replicate the cube points to issues that go far beyond simple drawing ability.
These tasks are designed to probe the frontal and parietal lobes, giving you critical data that helps differentiate between various types of cognitive decline.
Actionable Insight: A patient’s failure on the MoCA’s cube copy or clock draw isn't just a lost point; it's a specific flag for visuospatial and executive dysfunction. This insight is actionable, suggesting the need for further neurological investigation focused on the frontal-subcortical circuits, a step you might not take based on an MMSE score alone.
Memory: Registration vs. Delayed Recall
Both tests assess memory, but how they do it has significant implications for spotting mild cognitive impairment (MCI). The MMSE primarily tests registration and simple recall, whereas the MoCA challenges a patient's delayed recall without offering any hints.
Practical Example: In the MMSE, a patient repeats three words and then recalls them a few minutes later. If they can't remember, they get a categorical cue, like, "It was a type of fruit."
The MoCA, on the other hand, presents five words. After a delay filled with distractor tasks, it asks for recall without any cues. Cues are only offered as an optional second step to see if the memory was encoded but just hard to retrieve. Actionable Insight: A patient who can't recall the five MoCA words shows a more significant memory problem than one who just needs a prompt on the MMSE. This distinction helps differentiate between a retrieval issue (cues help) and a more serious encoding issue (cues don't help).
Language and Abstraction
The MMSE's language tasks are quite basic, focusing on naming common objects like a watch or a pencil and following simple commands. The MoCA's language and abstraction tasks are far more demanding, which is why they're so much more sensitive to subtle changes.
The MoCA includes:
Phonemic Fluency: The patient has to name as many words as they can that start with a specific letter (like "F") in one minute. This is a tough executive function task that requires mental flexibility and verbal retrieval strategies. A score of less than 11 words is a major red flag.
Abstraction: Patients are asked what two concepts have in common (e.g., "train and bicycle," "watch and ruler"). This tests conceptual thinking. A concrete answer like "they both have wheels" scores lower than an abstract one like "they are both forms of transportation."
It's these more complex tasks that explain why the MoCA consistently outperforms the MMSE in detecting early, subtle decline. In fact, studies mirroring Canadian neurodegenerative research protocols have found MoCA scores to be more discriminative across various clinical groups. This research emphasizes that the MoCA's inclusion of executive function and attention tasks—largely missing in the MMSE—allows it to spot impairments 20-30% earlier in some conditions. You can read the full study about these important findings on neurodegenerative disease screening protocols.
Understanding these domain-specific differences is what separates a novice from an expert in cognitive assessment. For a deeper dive, check out our guide on what is cognitive function and how these domains are all connected. By analyzing the pattern of errors, you move beyond a simple score to form a rich, evidence-based clinical hypothesis.
Sensitivity, Specificity, and the Ceiling Effect in Practice
Psychometric jargon like "sensitivity" and "specificity" can feel academic, but in the clinic, they have profound, real-world consequences. When you’re choosing between the Montreal Cognitive Assessment and the MMSE, these metrics are what separate a missed diagnosis from a false positive—and that choice directly shapes a patient's future.
The fundamental problem with the MMSE, particularly in primary care or outpatient settings, is its low sensitivity for mild cognitive impairment (MCI). This gives rise to its infamous ceiling effect, a frustrating phenomenon where people with genuine, early-stage deficits still score in the “normal” range. This is especially true for our patients with higher education or a lifetime of cognitive reserve.
A perfect score on an MMSE doesn't always mean everything is fine. More often than not, it just means the test was too easy to pick up the subtle cracks beginning to show.
The Danger of a High Ceiling
When a test has a high ceiling, it simply lacks the challenging questions needed to unmask subtle cognitive problems. This creates a dangerous illusion of security. A patient with emerging MCI is told everything is fine, which delays critical interventions, family discussions, and future planning.
Practical Example: The Retired Professor
Imagine a 72-year-old retired history professor. His family is worried. They've noticed he's having trouble with complex financial planning and has started repeating the same stories.
On the MMSE: He aces it, scoring a 29/30. He has no problem with orientation, simple registration, or basic recall. The test just isn't built to probe his slipping higher-level executive functions.
On the MoCA: The picture changes entirely. He stumbles on the abstraction task (like comparing a train and a bicycle), struggles with the Trail Making Test, and can only come up with seven words during the phonemic fluency task. His score is 22/30, clearly pointing to an impairment.
This is the ceiling effect in action. The MMSE gave a false sense of security, while the MoCA’s higher "cognitive ceiling" successfully brought the executive dysfunction—the very thing causing his real-world problems—to light.
Actionable Insight: The greatest risk of the MMSE's ceiling effect isn't just a missed diagnosis, but a delayed one. Research consistently shows a striking number of patients labelled "cognitively normal" by the MMSE are later reclassified as impaired by the MoCA. If a patient’s subjective complaints don't match their "normal" MMSE score, trust your clinical judgment and administer a MoCA.
Sensitivity and Specificity in Clinical Context
The choice between the MoCA and the MMSE really comes down to which risk you’re more willing to take in a given situation: missing a diagnosis (low sensitivity) or incorrectly flagging a healthy individual (low specificity).
Post-stroke cognitive assessment, a frequent challenge in Canadian healthcare, offers a powerful example. A comparative study of post-stroke patients found the MoCA-B was far more sensitive at detecting post-stroke cognitive impairment (PSCI). At a cutoff of <25, the MMSE's sensitivity was only 70.59%. In sharp contrast, the MoCA-B, with a cutoff of <23, reached a sensitivity of 85.71%.
Even more telling, of the 63 patients the MMSE had cleared as cognitively normal, nearly a third (29.8%) were reclassified as impaired by the MoCA-B. This starkly illustrates the MMSE’s tendency to miss the subtle deficits so common after a stroke.
At the end of the day, your choice between the Montreal Cognitive Assessment vs MMSE has to be driven by the clinical question at hand. If you’re screening for MCI or assessing a patient with a high cognitive reserve, the MoCA’s superior sensitivity is a must. It has the rigour to detect problems early.
While no single test is flawless, understanding the test-retest reliability and unique psychometric profiles of these tools helps you make a more informed and defensible clinical decision. The MMSE might still have its place in tracking the progression of established dementia, but for detection, the MoCA has become the clear standard.
Putting It All into Practice: Clinical Scenarios
Knowing the textbook differences between the Montreal Cognitive Assessment and the MMSE is one thing. Choosing the right tool under the pressure of a busy clinical day is another entirely. This is where the theory hits the clinic floor.
Making the right call isn't just about picking the test with the better psychometric profile. It's about a pragmatic decision that best serves the specific patient in front of you. By walking through a few common clinical vignettes, we can see how the patient's story and the core clinical question should drive your choice every time.

Scenario 1: The High-Functioning Patient with Subtle Concerns
The Patient: A 70-year-old retired engineer, "Mr. Chen," comes to your office at his daughter's urging. He reports some mild memory lapses—forgetting names, misplacing keys—but he’s still active, manages his own finances, and enjoys his hobbies. He just feels he’s “not as sharp as he used to be.”
Clinical Question: Are these subjective complaints just normal aging, or are they the first signs of Mild Cognitive Impairment (MCI)?
Recommended Tool: The Montreal Cognitive Assessment (MoCA) is the only real choice here.
Actionable Insight: Mr. Chen’s high educational and professional background all but guarantees the MMSE will fail you due to its ceiling effect. Using the MMSE would be a missed opportunity. The MoCA was built for exactly this situation, using its challenging executive function and delayed recall tasks to uncover the subtle slips his family is worried about. For any high-functioning patient with subtle complaints, default to the MoCA.
Scenario 2: Routine Monitoring in Established Dementia
The Patient: "Mrs. Dubois" is an 88-year-old resident in a long-term care facility. She was diagnosed with moderate Alzheimer's disease five years ago and needs help with most of her daily activities. Her care team just wants to do a routine quarterly cognitive check.
Clinical Question: Has there been a meaningful change in her cognitive baseline over the last three months?
Recommended Tool: The Mini-Mental State Examination (MMSE) is the pragmatic and efficient tool for the job.
Actionable Insight: Here, the goal isn't detection; it's longitudinal tracking. Mrs. Dubois would likely hit the "floor effect" on the MoCA, where the test is too difficult to measure real change. The MMSE's speed (5-10 minutes) and simplicity make it a useful, less taxing yardstick. A drop of a few points on the MMSE is a clear, easily communicated signal that her condition is progressing.
Scenario 3: Assessing Capacity After a Neurological Event
The Patient: "Ms. Garcia" is a 60-year-old accountant recovering from a subarachnoid hemorrhage. She feels she has recovered well and is anxious to return to her demanding job. Her employer needs a cognitive evaluation.
Clinical Question: Does she have lingering cognitive deficits, especially in executive function, that could put her or her clients at risk?
Recommended Tool: The Montreal Cognitive Assessment (MoCA) is non-negotiable.
Actionable Insight: A return-to-work evaluation is all about higher-order cognitive skills. The MMSE, with its glaring lack of executive function items, would be dangerously insufficient. The MoCA’s tasks (abstraction, fluency, attention) map directly onto the skills Ms. Garcia needs as an accountant. As research like the study on post-SAH screening confirms, the MoCA sees functional deficits the MMSE completely misses, making it the essential tool for capacity assessments.
Of course, a cognitive score also helps guide other recommendations. For many older adults, a clinician might suggest incorporating effective memory exercises for seniors to support cognitive health.
As these scenarios show, the "best" tool is always the one that best fits the clinical context. To add even more granular data to your assessments, schedule a demo of the Orange Neurosciences platform by contacting us today through our website.
Beyond the Screener: Why Digital Cognitive Assessment is the Next Step
Let's be honest. The debate between the Montreal Cognitive Assessment and the MMSE is important, but it keeps us focused on the inherent limits of paper-and-pen screeners. Both are just snapshots in time. They're vulnerable to who gives the test, how it's given, and whether the patient has seen it before. For any clinician who's ever wanted a deeper, more objective look at a patient's cognitive health, it's clear we need to move past these traditional tools.
This is where digital cognitive assessment comes in, and frankly, it's changing the game.

Platforms like the ones we're building at Orange Neurosciences offer a completely new way forward. Instead of a single score from a 10-minute test, you get a comprehensive, standardized cognitive profile. Think of it as getting the depth of a full neuropsych exam, but without the months-long wait times.
Getting Objective Data You Can Actually Trust
The biggest problem with paper tests is their subjectivity. We've all seen how small variations in how a test is administered can skew the results. Digital platforms eliminate that. Every instruction, every task, and every measurement is delivered the exact same way to every single patient. This consistency means the data you get is a true picture of their cognitive function, not an artifact of the testing process.
Practical Example: Take our OrangeCheck assessment. In under 30 minutes, it gives you a detailed look at six key cognitive domains. You get objective, granular data on specific functions like processing speed, working memory, and executive function. Actionable Insight: This level of detail allows you to build a care plan that’s genuinely tailored to that individual’s cognitive profile, moving beyond a simple "impaired" or "not impaired" label.
The Power of Gamified Tasks and Tracking Over Time
Another major headache with tools like the MoCA is keeping patients engaged. Worse, they can start to memorize the test, which makes re-testing almost useless. Digital assessments get around this with an engaging, gamified interface. These aren't just tests; they're interactive tasks that feel more like a game. This simple shift improves patient motivation and makes the data you collect that much more reliable.
This is what makes longitudinal tracking so powerful.
Establish a Real Baseline: You can set a detailed, multi-domain cognitive baseline for every new patient.
See the Change: Objectively measure how a patient’s cognition is changing over time, whether in response to treatment or as a disease progresses.
Re-test with Confidence: You can re-assess patients knowing that the varied, engaging tasks prevent the practice effects that plague paper screeners.
Actionable Insight: The real power here is moving cognitive evaluation from a one-off event to a continuous part of patient care. When you have objective, repeatable data, you can make clinical decisions in real-time and track cognitive health with a precision that paper screeners just can't deliver.
While screeners do a good job of flagging a potential problem, digital tools give you the deep insights you need to actually do something about it. They are the logical next step in modern cognitive care, providing the robust data needed for confident diagnosis and effective treatment planning. You can explore more about what makes these tools so effective in our guide to cognitive assessment online.
To see for yourself how digital neuropsychiatry can elevate your practice, email us for information or visit our website to request a demo of the Orange Neurosciences platform today.
Here are some of the most common questions that come up in the clinic when clinicians are weighing the MoCA against the MMSE. Let's walk through the practical answers to help you sharpen your cognitive screening strategy.
Is the MoCA Always the Better Choice?
Not necessarily. It's a classic case of using the right tool for the right job.
While the MoCA is undeniably superior for picking up on mild cognitive impairment (MCI), thanks to its higher sensitivity and more challenging tasks, the MMSE still has its place. For patients with moderate-to-severe established dementia, the MMSE is often the more pragmatic and efficient choice. Its simplicity and speed are perfect for routine tracking of cognitive decline where the goal isn't subtle detection but monitoring a known condition. Actionable Insight: The clinical goal dictates the tool. Detection = MoCA. Tracking established decline = MMSE.
How Should I Adjust Scores for Education Level?
Adjusting for education is a critical step for accuracy, but the two tests handle it very differently.
For the MoCA: The rule is straightforward. You add one point to the final score for any patient who has 12 years or less of formal education. This is a built-in correction to help account for potential educational bias.
For the MMSE: This is one of its noted limitations. There isn't a single, universally accepted standard for an education adjustment. While various local norms and research-based corrections exist, the official test lacks a built-in rule like the MoCA's.
What Training Is Required to Administer the MoCA?
Yes, this is a key differentiator. To administer and score the MoCA, mandatory training and certification are required.
This process, which can be completed online, is in place to ensure administration is standardized across all settings. That consistency is crucial for the reliability and validity of the test results. This is a significant departure from the MMSE, which has far less formal training requirements.
Can These Tests Actually Diagnose Dementia?
This is a point that can't be stressed enough: No. Both the MoCA and the MMSE are screening tools, not diagnostic instruments.
Think of them as a vital first alert. A low score signals a high probability of cognitive impairment and tells you it's time for a full diagnostic workup. Actionable Insight: A low score is not a diagnosis; it's the trigger for action. That comprehensive evaluation is what leads to a diagnosis and may include everything from neuroimaging and lab tests to a full neuropsychological assessment.
These screeners are brilliant at flagging that something might be wrong, but they boil a complex cognitive picture down to a single score. To get the granular, objective data needed for precise care planning, you need to go deeper. The Orange Neurosciences platform provides a detailed cognitive profile in under 30 minutes, giving you the kind of insight that moves you beyond a simple score. Visit our website or email us to explore how our digital tools can support your practice.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation