Guide to moca assessment vs mmse: A Clinician's Cognitive Screening Overview
Feb 21, 2026

When it comes to the MoCA assessment vs MMSE, the right choice really boils down to your clinical goal. Think of it this way: The Montreal Cognitive Assessment (MoCA) is your go-to for picking up on subtle deficits and what's known as Mild Cognitive Impairment (MCI). On the other hand, the Mini-Mental State Examination (MMSE) has traditionally been used to track the progression of moderate to severe dementia.
Choosing the Right Cognitive Screener
Picking the right cognitive screener is more than just a preliminary step; it sets the stage for the entire patient assessment. It's not about getting a number—it’s about asking the right questions to uncover specific, often subtle, changes in cognition. Your choice between the MoCA and the MMSE can make all the difference in early detection and, consequently, timely intervention.
Let’s take a common clinical scenario: a patient comes in with subjective memory complaints but seems to be managing their daily life just fine. This is precisely where the MMSE, with its simpler structure, can fall short. Its "ceiling effect" means a patient can score perfectly yet still have underlying issues the test just isn't designed to find. The MoCA was created specifically to fill this exact gap.
Key Distinctions at a Glance
The core difference between the two screeners is their complexity and focus. The MoCA deliberately includes more challenging tasks that probe executive function, abstract thinking, and complex visuospatial skills. These are the very domains where the first signs of cognitive decline often surface.
The MoCA's design specifically targets early-stage cognitive changes that the MMSE often misses, making it a more powerful instrument for timely and accurate screening in modern clinical practice.
Here’s a quick breakdown of the key differences before we get into the nitty-gritty of each test. It's also worth noting that these screeners are part of a wider ecosystem of comprehensive mental health assessment tools that clinicians have at their disposal.
Feature | Montreal Cognitive Assessment (MoCA) | Mini-Mental State Examination (MMSE) |
|---|---|---|
Primary Use Case | Detecting Mild Cognitive Impairment (MCI) | Screening for moderate to severe dementia |
Sensitivity for MCI | High (around 90% sensitivity) | Low (often below 25% sensitivity) |
Key Domains Tested | Executive Function, Visuospatial, Memory | Orientation, Attention, Basic Recall |
Administration Time | Approximately 10–15 minutes | Approximately 7–10 minutes |
Ultimately, choosing between the MoCA and MMSE isn’t about which one is "better," but which tool’s strengths align with your patient’s presentation and the clinical question at hand. Modern digital platforms, like the ones we’ve developed at Orange Neurosciences, build on these foundational screening principles to offer even more precise insights. You can explore our advanced cognitive assessments to see how they support clinicians in making better-informed decisions.
To really get to the heart of the MoCA vs. MMSE comparison, you have to look at where they came from. Each tool was built to solve a different problem, in a different era of medicine. This history is the key to understanding why they function so differently in a modern clinic.
The Mini-Mental State Examination (MMSE) came first, way back in 1975. Its job was simple: give clinicians a quick, straightforward way to screen for and track clear-cut dementia. It was designed to be easy, focusing heavily on basic things like knowing the date and location.
For its time, the MMSE was a big deal. It gave doctors a standardized way to put a number on cognitive impairment when there wasn't much else available. But that simplicity is exactly what holds it back today, now that our focus has shifted to catching problems much, much earlier.
The Rise of the MoCA for Early Detection
As our understanding of cognitive decline evolved, a huge gap appeared. Clinicians realized the MMSE was consistently missing Mild Cognitive Impairment (MCI)—that critical grey area between normal aging and dementia. Patients were acing the MMSE while hiding subtle but very real cognitive issues.
This clinical blind spot led directly to the development of the Montreal Cognitive Assessment (MoCA) in 1996. The MoCA was engineered from the ground up to fix the MMSE's shortcomings. It deliberately includes more complex tasks that push the very cognitive domains where the first signs of trouble tend to show up.
The core difference is a philosophical one. The MMSE was built to confirm significant cognitive loss. The MoCA was built to uncover the suspicion of it, long before it becomes obvious to everyone.
For instance, the MoCA adds tasks that really challenge the brain in ways the MMSE doesn't:
Executive Function: It includes things like the Trail Making Test B (alternating between numbers and letters) and abstraction (explaining how a train and a bicycle are alike).
Visuospatial Skills: The MoCA asks for more than just copying a simple shape; it requires drawing a 3D cube and a clock showing a specific time.
Higher-Level Language: It tests verbal fluency by asking the patient to name as many words as they can that start with a certain letter in one minute.
These tasks make the MoCA a much more sensitive tool for spotting the earliest signs of trouble. It’s simply a more modern instrument. If you're planning to use it, our guide offers detailed Montreal Cognitive Assessment instructions to ensure you’re administering it correctly.
A Tale of Two Sensitivities
The real-world difference between these two design philosophies is staggering. When it comes to detecting MCI, the MoCA is just in another league. Study after study shows the MoCA’s sensitivity for MCI hovers between 90% and 100%. In those same studies, the MMSE’s sensitivity for MCI can plummet to as low as 18%.
Think about that. For every ten patients with MCI, the MoCA will correctly flag at least nine of them. The MMSE might only catch two. This is the foundational difference that explains why choosing the right tool has such a profound impact on proactive care and patient outcomes.
Comparing Cognitive Domains And Task Structures
When you compare the MoCA and the MMSE, the real story isn't just the final score. It's in the tasks. The differences between them aren't merely academic; they show a fundamental split in what each screener is designed to uncover. While they're both 30-point assessments, the cognitive ground they cover is vastly different, with the MoCA probing deeper into functions the MMSE barely touches.
This distinction is absolutely critical for early detection. It's not uncommon for a patient to score perfectly on the MMSE’s simpler items while significant, yet subtle, cognitive deficits go completely unnoticed. The MoCA’s design directly confronts this very issue by including tasks that are more demanding and better reflect the challenges of real-world cognition.
So, let's break down exactly where their task structures diverge and what these differences truly mean in a clinical setting.
Memory: A Tale Of Two Recalls
The most telling contrast between the two is how they handle short-term memory—a function often hit early in conditions like Alzheimer's disease.
MMSE Task: It asks the person to recall three unrelated words after a short delay. This is a pretty low-demand task that many people with amnestic MCI can still pass without trouble.
MoCA Task: The MoCA ramps up the difficulty quite a bit. It uses a list of five words and has a longer delay before asking for recall. This increases the cognitive load, making it much harder for someone with early memory deficits to succeed.
For example, a patient might easily remember "apple, table, penny" on the MMSE. But when faced with the MoCA’s list of "face, velvet, church, daisy, red," the added complexity might expose a subtle memory consolidation problem that the MMSE would have missed entirely.
Executive Function: The MoCA's Defining Advantage
Perhaps the single biggest gap the MoCA fills is its assessment of executive functions. This set of higher-order skills—planning, problem-solving, and mental flexibility—is almost entirely absent from the MMSE. This is a massive limitation, as executive dysfunction is a core feature of many neurodegenerative disorders.
The MoCA’s inclusion of specific executive function tasks is its single greatest advantage over the MMSE. It provides a critical window into frontal lobe function that is essential for detecting non-memory-related cognitive decline.
To see this in action, just look at these specific tasks:
Abstraction: The MoCA asks the person to explain the similarity between two items (e.g., "How are a train and a bicycle alike?"). This tests abstract reasoning, a skill the MMSE doesn't evaluate at all.
Trail Making Test (Part B): This task requires connecting a sequence of numbers and letters in alternating order (1-A-2-B-3-C...). It’s a classic neuropsychological test of cognitive flexibility and processing speed.
Verbal Fluency: The patient must name as many words as they can that start with a specific letter in 60 seconds. This is a great measure of spontaneous word production and mental organisation.
These tasks provide incredibly valuable data that can help differentiate between different types of dementia. If you're looking for more ways to evaluate this critical domain, you can learn more by checking out our guide on how to test for executive dysfunction.
Visuospatial Skills: From Simple Shapes To 3D Construction
Both tests include visuospatial tasks, but again, the level of complexity reveals their different purposes.
MMSE Task: The patient is asked to copy two intersecting pentagons. This is a relatively simple, two-dimensional figure-copying task.
MoCA Task: The MoCA requires two much more complex drawings. The patient has to draw a clock showing a specific time (ten past eleven) and copy a three-dimensional cube.
Here’s a practical example of why this matters. A 72-year-old patient might successfully draw the intersecting pentagons on the MMSE and get full points. But when asked to draw the MoCA’s cube, they might struggle with perspective, producing a flattened or distorted shape. This specific difficulty can point to a subtle decline in visuospatial constructional skills that the MMSE’s simpler task wasn't challenging enough to reveal. Likewise, placing the clock hands correctly requires both visuospatial planning and number comprehension, making it a much richer cognitive task.
MoCA vs MMSE Domain Coverage and Task Complexity
The table below provides a side-by-side look at how the cognitive domains stack up. Notice how the MoCA consistently introduces a higher level of complexity, which is key to its sensitivity for milder impairments.
Cognitive Domain | MMSE Task Example | MoCA Task Example | Clinical Significance of Difference |
|---|---|---|---|
Short-Term Memory | Immediate and delayed recall of 3 words. | Delayed recall of 5 words (no cues). | The MoCA's higher word count and longer delay are more sensitive to subtle memory consolidation deficits characteristic of early Alzheimer's. |
Visuospatial Skills | Copying two intersecting pentagons. | Clock drawing (to a specific time) and cube copying (3D). | MoCA's tasks are more complex, assessing planning, number comprehension, and 3D perception, which can reveal parietal lobe dysfunction. |
Executive Function | Essentially none. | Trail Making Test (B), verbal fluency, and abstraction. | This is the MoCA's biggest strength. It directly assesses frontal lobe functions that are crucial for detecting non-amnestic dementias. |
Attention | Serial 7s or spelling "world" backward. | Digit span (forward and backward), vigilance test (tapping for letter 'A'). | The MoCA's tasks are more varied and demanding, testing different aspects of attention, including sustained attention and working memory. |
Language | Naming two objects, following a 3-stage command, repeating "no ifs, ands, or buts." | Naming 3 less common animals, repeating complex sentences. | MoCA uses less common items and more complex sentences to reduce the ceiling effect and better detect subtle aphasias. |
Orientation | Orientation to time and place (10 points). | Orientation to time and place (6 points). | Both tests assess this well, but the MMSE places a heavier scoring weight on it. |
Ultimately, while both tools have their place, the MoCA’s design provides a much more detailed and nuanced picture of a person's cognitive abilities, especially when deficits are not yet severe.
Interpreting Scores and Psychometric Properties
Getting the final number on a MoCA or MMSE report is just the first step. The real skill lies in knowing what that number means within the context of each test’s unique design. While both assessments are scored out of 30, the clinical story behind those points can be vastly different, especially when you look at their sensitivity and specificity.
A raw score by itself doesn't tell you much. Both the MoCA and MMSE often use a score below 26 as a general cut-off to signal that something needs a closer look, but that’s where the similarities end.
One of the MoCA's most practical features is how it accounts for educational background. It recommends adding one point to the total score for anyone with 12 years or less of formal education. The standard MMSE doesn't have this built-in adjustment, a flaw that can lead to false positives and misinterpretations for people with lower educational attainment.
Sensitivity and The Problem of Ceiling Effects
When you put the MoCA assessment vs MMSE head-to-head, sensitivity is a game-changer. Sensitivity is a test's ability to correctly flag individuals who do have a cognitive impairment. This is where the MoCA shines, largely because it was built specifically to overcome the MMSE's well-known "ceiling effect."
A ceiling effect is what happens when a test is too easy. Highly educated or high-functioning individuals can ace the MMSE even when they have genuine, early-stage cognitive deficits. The test isn't challenging enough to catch subtle problems, resulting in a false negative that can provide a dangerous sense of reassurance and delay a crucial diagnosis.
A normal score on the MMSE does not reliably rule out Mild Cognitive Impairment. The MoCA's higher cognitive demand provides a much more accurate picture, reducing the risk of missing an early diagnosis due to ceiling effects.
This isn't just a statistical nuance; it has profound real-world consequences. It means the MMSE might completely miss the very first signs of a neurodegenerative condition—that critical window where interventions could be most effective.
A Practical Scenario in Scoring
Let's walk through a common clinical scenario to see how this plays out.
Patient Profile: A 68-year-old retired accountant with a master's degree. He complains of "mental fogginess" and occasionally misplacing important documents but is otherwise managing his daily life just fine.
MMSE Result: He scores 28/30. This is comfortably above the cut-off of 26 and is considered well within the normal range. Based on this result alone, a clinician might conclude there's no significant cognitive issue.
MoCA Result: The same patient scores 24/30. He lost points on the delayed five-word recall, struggled with the cube drawing, and couldn't complete the Trail Making B task correctly. This score falls below the <26 cut-off, strongly suggesting MCI.
This is a classic example of the MMSE's ceiling effect in action. The MoCA’s more difficult tasks targeting executive function and visuospatial skills picked up on deficits the MMSE simply couldn't detect. The concerning MoCA score would trigger a neurological referral that the "normal" MMSE score would have prevented. For a deeper dive into what these numbers mean, you can review our guide on MoCA score interpretation.
Context-Specific Cut-Offs and Accuracy
It’s also important to remember that the "best" cut-off score isn't set in stone; it can change depending on the clinical situation. Research shows that the diagnostic accuracy of the MoCA versus the MMSE varies significantly across different conditions and stages of disease.
For example, one study looking at cognitive impairment after a specific medical event found that the optimal MoCA cut-off was ≤18 shortly after the event and ≤22 a year later. In contrast, the MMSE cut-off remained ≤24 at both times. The diagnostic accuracy for these adjusted scores ranged from 80% to 92%. You can read the full research about these findings to see how cut-offs can be adapted.
This really drives home the point that interpreting scores is not a one-size-fits-all process. The MoCA's psychometric profile gives clinicians a more flexible and sensitive instrument, especially when tracking the subtle changes that mark early-stage cognitive decline.
Deciding Between MoCA and MMSE in Clinical Practice
The theory behind the MoCA and MMSE is one thing, but applying it in a bustling clinic is a whole different ball game. Picking the right screener isn't just an academic exercise—it's a hands-on decision that shapes patient care, how accurately we diagnose, and how quickly we can intervene. The real skill is matching the screener's strengths to the specific clinical question you need to answer for the person sitting in front of you.
When it comes to the moca assessment vs mmse debate, we need to reframe the question. Instead of asking, "Which test is better?" we should be asking, "Which test is better for this particular patient, right now?" The right answer always depends on their specific complaints, medical history, and what we're trying to accomplish with the assessment.
This simple flowchart can help visualize that initial thought process, based on how significant the patient's concerns are.
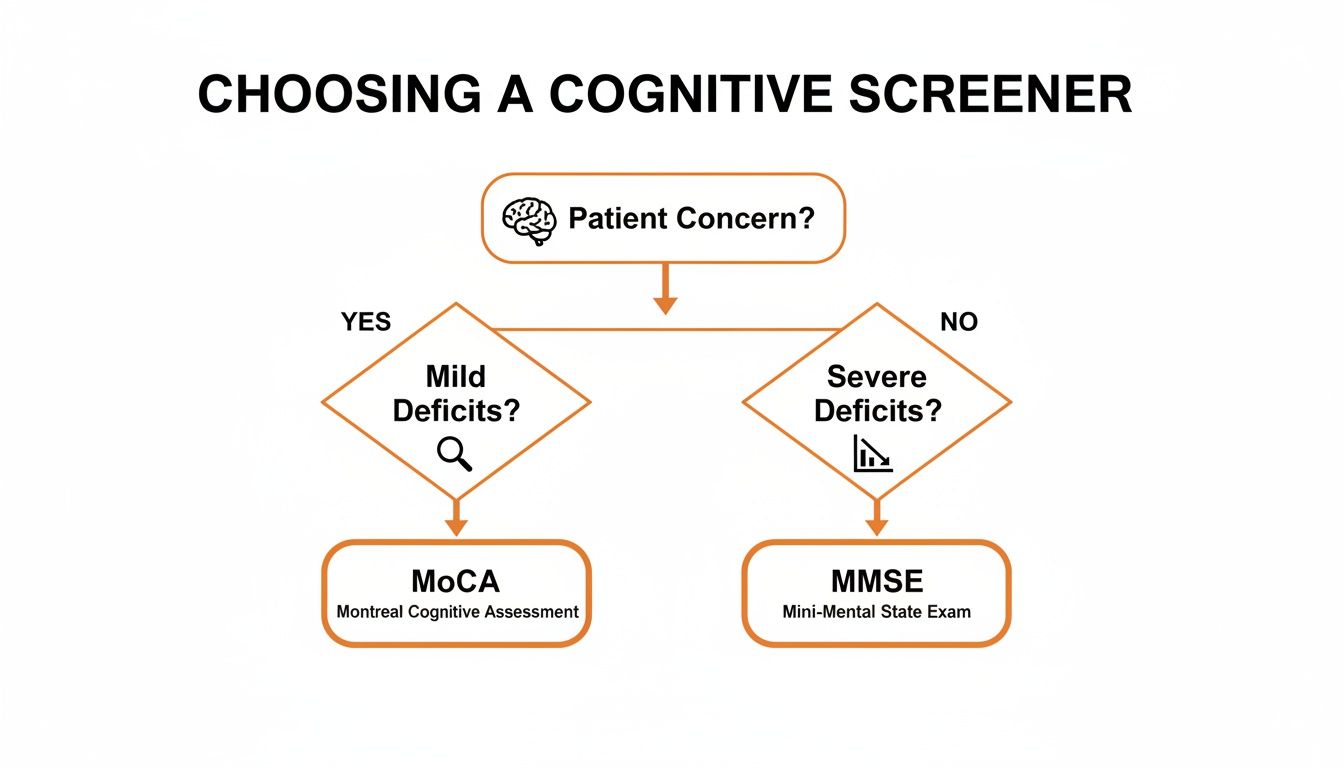
As you can see, the choice often comes down to a fundamental question: are we hunting for subtle, early-stage deficits, or are we tracking more obvious, advanced cognitive decline?
When to Choose the MoCA
The Montreal Cognitive Assessment really shines when your main job is detection. It was built from the ground up to catch the kinds of subtle slip-ups that the MMSE was never designed to find.
Think about these real-world scenarios where the MoCA is the obvious choice:
Subjective Memory Complaints: You have a 65-year-old patient who says they feel more forgetful and "foggy," but they're still managing their day-to-day life just fine. An MMSE would likely come back normal, giving everyone a false sense of security. The MoCA, with its tougher memory and executive function tasks, is crucial for digging deeper to see if these complaints are the first signs of Mild Cognitive Impairment (MCI).
Suspected Non-Memory Issues: For conditions like Parkinson's disease, cognitive troubles often show up as problems with executive function or visuospatial skills, not memory loss. Here, the MoCA is invaluable. Its specific tasks, like the Trail Making Test and cube copy, give you a direct look into these non-memory domains.
Post-Stroke Assessment: After a stroke, a patient's cognitive profile can be incredibly complex. The MoCA helps pinpoint specific deficits in attention, language, and executive function—information that is absolutely vital for putting together an effective rehabilitation plan.
Actionable Insight: Use the MoCA as your default screener for any patient presenting with new, mild, or subjective cognitive complaints. The resulting score provides a solid baseline and helps you decide if a referral for deeper neuropsychological testing is warranted.
When the MMSE Is Still a Practical Option
Even with its known blind spots for MCI, the Mini-Mental State Examination still has a role to play. In certain clinical situations, its simplicity and speed are exactly what you need.
Here’s when the MMSE might be the more sensible tool:
Tracking Established Dementia: For someone in long-term care with a confirmed diagnosis of moderate Alzheimer's, the goal is often to monitor their rate of decline. The MMSE is quick to do and can effectively track major shifts over time without causing undue frustration for a patient who is already severely impaired.
Bedside Screening in Acute Care: In a busy hospital ward, you might need a quick cognitive baseline for a patient who is very ill or tires easily. The MMSE’s brevity—often taking less than 10 minutes—is a huge plus. The goal isn't a detailed diagnosis, but a rapid snapshot of their overall cognitive function.
Severe Cognitive or Physical Impairments: If a patient has severe aphasia, vision problems, or motor limitations that make the MoCA's complex tasks impossible, the MMSE’s simpler verbal and orientation questions might be the only way to get any cognitive data at all.
Considering Population Factors in Your Choice
Beyond the clinical picture, patient-specific factors like education and cultural background have to be part of the equation.
The MoCA includes a one-point adjustment for individuals with 12 years or less of education. This is a built-in feature designed to reduce educational bias, making it a fairer tool for diverse populations. The MMSE, which lacks this formal adjustment, is more likely to misclassify people with lower educational attainment as being impaired.
On top of that, language and cultural background can affect performance. When working with patients from different cultures, a clinician needs to be aware of how items like naming a lion, rhino, or camel on the MoCA might be influenced by someone's life experiences. A good clinician will always interpret scores within the full context of the patient's personal history.
Large-scale research backs this up. One study involving nearly 5,000 subjects found the prevalence of MCI was significantly higher when screened with the MoCA (36.2%) versus the MMSE (28.6%). The MoCA also demonstrated greater variability in scores, suggesting it’s better at capturing the full spectrum of cognitive abilities. You can discover more insights about these cognitive assessment findings to see the statistical breakdown. This data just reinforces that the MoCA is a more powerful tool for identifying cognitive differences in a population.
Ultimately, navigating the moca assessment vs mmse choice comes down to sound clinical judgment. By weighing the patient's presentation, the goal of the assessment, and their individual background, you can confidently choose the tool that will give you the most accurate and useful information. For a deeper analysis that goes beyond screening, platforms like those from Orange Neurosciences can provide that next level of objective data.
Moving Beyond Screening with Digital Cognitive Tools

The whole MoCA assessment vs MMSE debate really brings a crucial point into focus: a single screening is just the beginning of the story, not the end. These pen-and-paper tests are absolutely invaluable for flagging potential red flags, but they do have their limits. For one, if you repeat them too soon, you run into "practice effects" that can skew the results. They also don't really capture fine-grained data like processing speed or sustained attention with the objective precision we need.
This is exactly where digital cognitive tools come in. They aren't here to replace those foundational screeners but to build on them, offering a much deeper and more dynamic look into a person's cognitive profile. It’s about moving beyond a simple score to a multi-faceted analysis. Platforms like Orange Neurosciences are designed to bridge that exact gap, providing a detailed, evidence-based follow-up to an initial screening.
Enhancing Clinical Decision Making
Think about this real-world scenario: a patient scores a borderline 25 on the MoCA. That score raises a clinical question, but it doesn't really give you a clear answer on what to do next. Instead of putting them on a months-long waitlist for a full neuropsychological workup, a clinician can use a digital platform right away to get a more comprehensive and objective cognitive snapshot.
This provides immediate, actionable data across multiple domains. It’s a powerful next step, and the future is likely to see even more sophisticated approaches, like the AI healthcare assessment tools being developed today.
Actionable Insight: After a concerning MoCA or MMSE result, use a digital assessment to get objective, longitudinal data. This allows you to track subtle changes in cognition over time, helping you fine-tune treatment plans and make data-driven decisions without lengthy delays.
Practical Benefits of Integration
Bringing digital platforms into a clinical workflow offers some serious practical wins for busy practices and their patients.
Objective Data: AI-driven systems can measure reaction times down to the millisecond. This gives you objective data that isn't influenced by administrator bias or human error.
Longitudinal Tracking: Assessments can be easily re-administered, allowing for consistent monitoring of cognitive function. This makes it far easier to track disease progression or see if an intervention is actually working.
Integrated Therapy: Many platforms don't just assess; they also offer engaging, game-based cognitive therapy. This creates a seamless loop of evaluation, intervention, and support.
For clinicians who are committed to providing faster, better-informed, and more personalized care, these tools are the logical next step. They elevate your practice from a simple screening to a powerful, data-driven care strategy. You can learn more about making this transition by exploring our guide on cognitive assessment online.
Common Questions About the MoCA and MMSE
When you're deciding between the MoCA and the MMSE, practical questions always come up. How long will it take? Is it right for this patient? Getting these answers straight is key to choosing the right tool for your clinic and the person sitting in front of you.
Let's clear up some of the most common queries, moving past the textbook differences to give you the confidence to use these screeners effectively day-to-day.
Can The MoCA Be Used for Patients with Low Education Levels?
Yes, it can, and this is one of its key strengths. The MoCA was designed with educational equity in mind, including a standard one-point correction for anyone with 12 years or less of formal education.
This simple adjustment helps reduce the bias that can creep in with education level, making the test more accurate across a wider range of people. For example, if a patient with 10 years of school scores a 25, their adjusted score becomes 26 — right at the normal cut-off. The standard MMSE doesn’t have a similar built-in fix, which can be a real drawback.
How Long Does Each Test Typically Take to Administer?
Time is always a factor in a busy practice, and there’s a clear difference here.
The MMSE is the quicker of the two, usually taking about 7-10 minutes to run through. Its straightforward design makes it fast to administer.
The MoCA takes a bit longer, generally between 10-15 minutes. That extra time is spent on more nuanced tasks like the Trail Making Test and cube drawing, which are precisely what give it the power to dig deeper into cognitive function.
Is The MoCA Always Better Than The MMSE?
Not always. It really depends on what you’re trying to do. For detecting mild cognitive impairment (MCI) and the very first signs of dementia, the MoCA is hands-down the superior tool. Its sensitivity to subtle deficits makes it the go-to for an initial workup when a patient reports concerns.
But for tracking cognitive changes in someone with already diagnosed moderate to severe dementia, the MMSE is often more practical. It's simple enough to avoid causing frustration for a person with significant impairment while still being a reliable way to spot major shifts in their condition over time.
Are There Official Training Requirements for Administering These Tests?
Yes, and this is crucial for getting results you can trust. To administer the MoCA, you need to complete a mandatory online training and certification program. This ensures everyone administers and scores the test in a standardized way, which is vital for its validity.
For the MMSE, the training isn't as formally standardized, but professional familiarity and adherence to the protocol are still strongly recommended. Proper administration is key to accurately interpreting the scores and making sound clinical judgments.
A screening is just the start. For a deeper, objective analysis of cognitive function that goes beyond a single score, Orange Neurosciences offers AI-powered assessments and targeted therapy. Our platform provides the granular data you need to make faster, better-informed care decisions. Explore how our digital tools can augment your clinical practice at https://orangeneurosciences.ca or sign up for our newsletter to get the latest clinical insights delivered directly to your inbox.

Orange Neurosciences' Cognitive Skills Assessments (CSA) are intended as an aid for assessing the cognitive well-being of an individual. In a clinical setting, the CSA results (when interpreted by a qualified healthcare provider) may be used as an aid in determining whether further cognitive evaluation is needed. Orange Neurosciences' brain training programs are designed to promote and encourage overall cognitive health. Orange Neurosciences does not offer any medical diagnosis or treatment of any medical disease or condition. Orange Neurosciences products may also be used for research purposes for any range of cognition-related assessments. If used for research purposes, all use of the product must comply with the appropriate human subjects' procedures as they exist within the researcher's institution and will be the researcher's responsibility. All such human subject protections shall be under the provisions of all applicable sections of the Code of Federal Regulations.



© 2026 by Orange Neurosciences Corporation